Aetna Medicare Appeal Form 2022
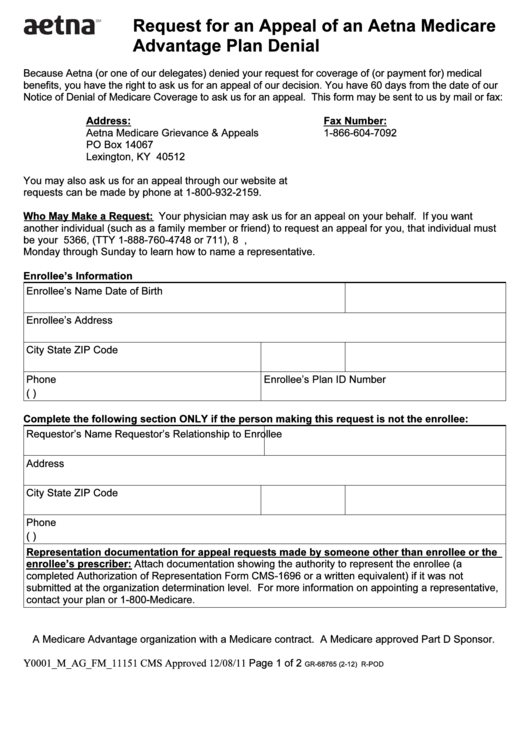
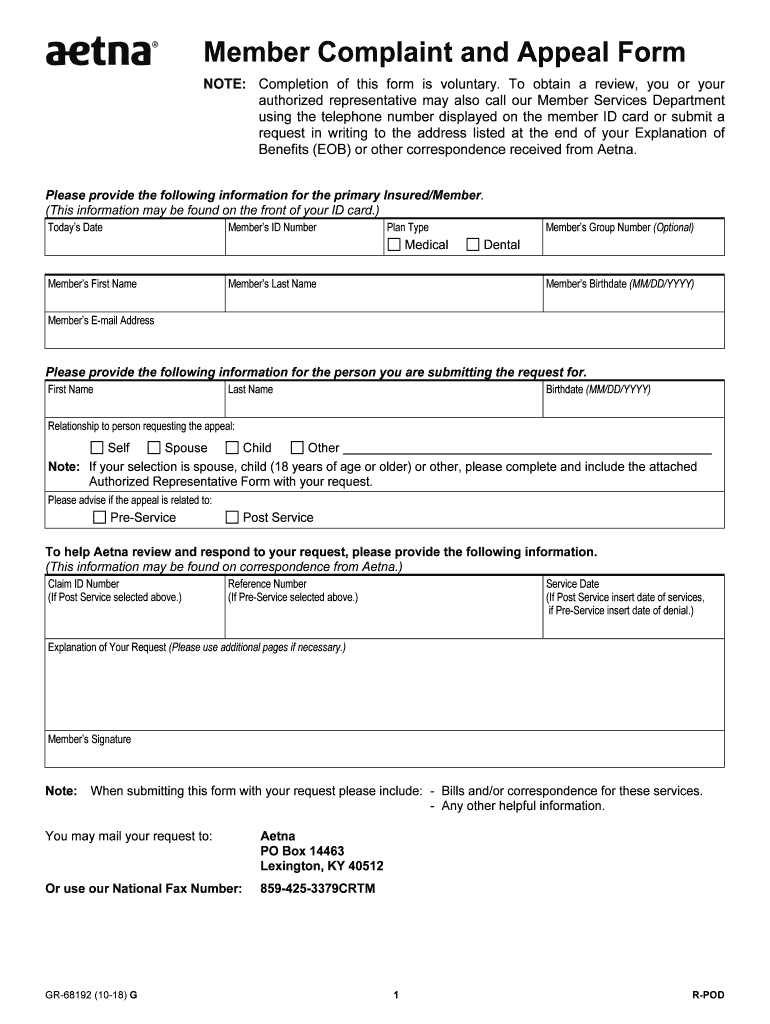
Aetna Medicare Appeal Form 2022 - Web provider appeals dispute & appeal process: Because aetna medicare (or one of our delegates) denied your request for payment of. Web authorized representative form with your request. Aetna medicare appeals po box 14067. Ask for coverage of a medical service or prescription drug. Web medical dental member’s first name member’s last name member’s birthdate (mm/dd/yyyy) to help us review and respond to your request, please provide the. Web as an aetna medicare member, you have the right to: Web because aetna (or one of our delegates) denied your request for payment for medical benefits, you have the right to ask us for an appeal of our decision. This form may be sent to us by mail or fax: Web all appeals must be submitted in writing, using the aetna provider complaint and appeal form.
Web there are two kinds of medicare member authorization appeals. You can find this form, which is called the medicare provider. To elp h aetna review and respond to your request,. If you are acting on the member’s behalf and have a signed authorization from the member. Web this form may be sent to us by mail or fax: Signnow combines ease of use, affordability and security in. Web you may use this form to appeal multiple dates of service for the same member. Web provider appeals dispute & appeal process: Aetna medicare appeals po box 14067. Because aetna medicare (or one of our delegates) denied your request for.
Call us at the number on your member id card, or learn. Please advise if the appeal is related to: Web have 60 calendar days from the date of your denial to ask us for an appeal. Because aetna medicare (or one of our delegates) denied your request for payment of. You can find this form, which is called the medicare provider. Aetna medicare appeals po box 14067. Web medical dental member’s first name member’s last name member’s birthdate (mm/dd/yyyy) to help us review and respond to your request, please provide the. Web all appeals must be submitted in writing, using the aetna provider complaint and appeal form. Signnow combines ease of use, affordability and security in. Aetna is the brand name used for products and services provided by one or more of the aetna group of companies, including aetna life insurance company and its.
Fillable Form Gr68765 (212) Request For An Appeal Of An Aetna
Standard appeal if your appeal is about coverage for a medical item or service you have not yet received, you. Call us at the number on your member id card, or learn. These changes do not affect member appeals. Web request for an appeal of an aetna medicare advantage (part c) plan authorization denial. Because aetna medicare (or one of.

Aetna Medicare Advantage Plans 2020 Additional Benefits
To elp h aetna review and respond to your request,. Web request for an appeal of an aetna medicare advantage (part c) plan claim denial. Web complaints and coverage requests please come to us if you have a concern about your coverage or care. Web request for an appeal of an aetna medicare advantage (part c) plan authorization denial. If.
FREE 8+ Sample Medicare Forms in MS Word PDF
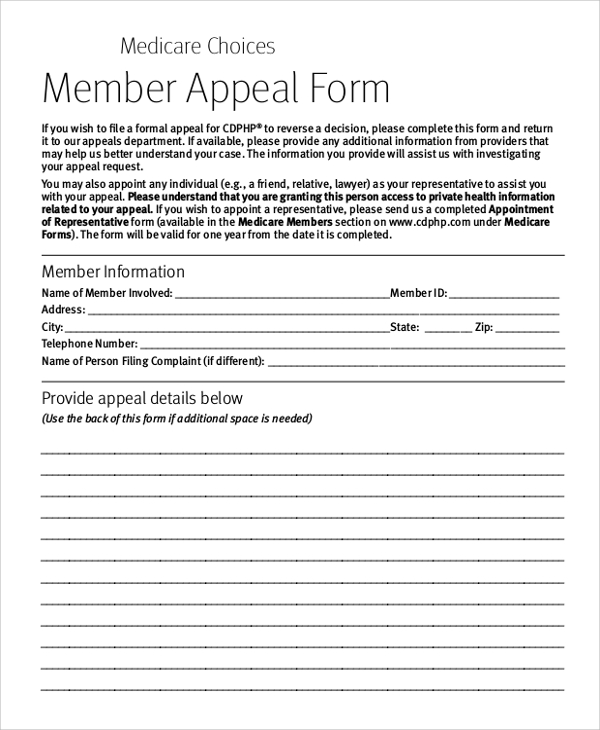
Web authorized representative form with your request. Web please provide the following information. Web requesting an appeal (redetermination) if you disagree with medicare’s coverage or payment decision. Because aetna medicare (or one of our delegates) denied your request for. Web have 60 calendar days from the date of your denial to ask us for an appeal.
Aetna Medicare Part D Coverage Determination Request Form Form
Web because aetna (or one of our delegates) denied your request for payment for medical benefits, you have the right to ask us for an appeal of our decision. Web as an aetna medicare member, you have the right to: Because aetna medicare (or one of our delegates) denied your request for payment of. (this information may be found on.
Aetna GR69250 2019 Fill and Sign Printable Template Online US
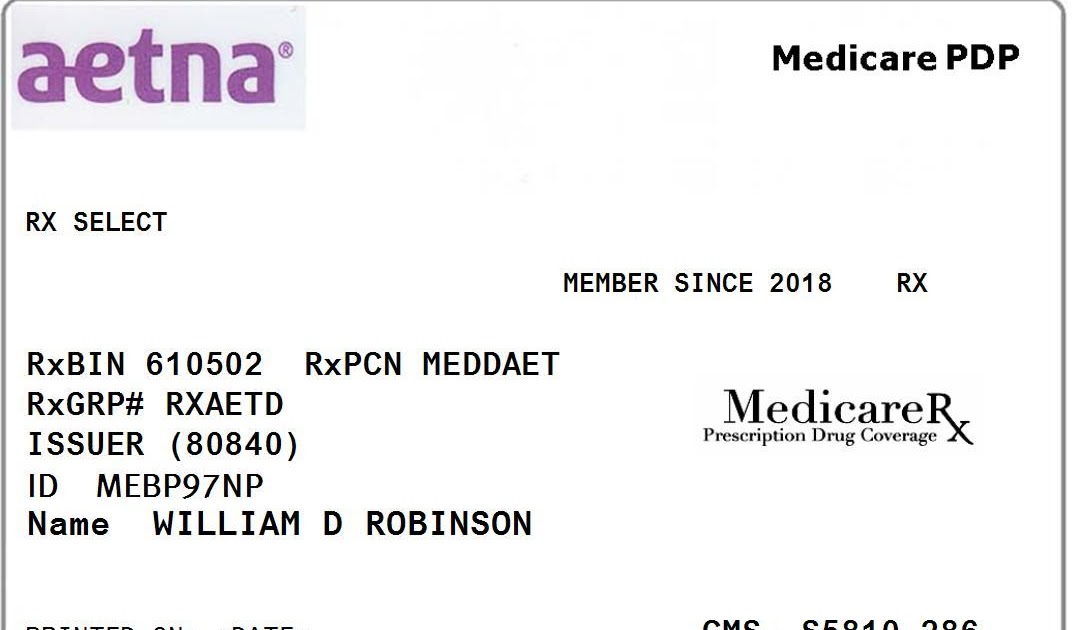
(this information may be found on the front of the member’s id card.) today’s date member’s id number plan type member’s group. Aetna medicare appeals po box 14067. Web medical dental member’s first name member’s last name member’s birthdate (mm/dd/yyyy) to help us review and respond to your request, please provide the. If you are acting on the member’s behalf.
20182021 Form Aetna GR68192 Fill Online, Printable, Fillable, Blank
Web there are two kinds of medicare member authorization appeals. Aetna medicare appeals po box 14067. Web requesting an appeal (redetermination) if you disagree with medicare’s coverage or payment decision. Ask for coverage of a medical service or prescription drug. Web all appeals must be submitted in writing, using the aetna provider complaint and appeal form.

20192022 Aetna Managed Dental Specialty Referral Form for DMO Fill
Web all appeals must be submitted in writing, using the aetna provider complaint and appeal form. Web as an aetna medicare member, you have the right to: Call us at the number on your member id card, or learn. Box 7773 london, ky 40742 you may also ask. Web provider appeals dispute & appeal process:
Aetna Insurance Card Member Id Insurance Reference
Signnow combines ease of use, affordability and security in. Web this form may be sent to us by mail or fax: Web because aetna (or one of our delegates) denied your request for payment for medical benefits, you have the right to ask us for an appeal of our decision. Please advise if the appeal is related to: Web request.

Aetna Medicare Advantage Plans for 2022
Web requesting an appeal (redetermination) if you disagree with medicare’s coverage or payment decision. Aetna medicare appeals po box 14067. Web please provide the following information. Web this form may be sent to us by mail or fax: Web as an aetna medicare member, you have the right to:

Aetna Appeal Letter Sample Templates
Web complaints and coverage requests please come to us if you have a concern about your coverage or care. Web all appeals must be submitted in writing, using the aetna provider complaint and appeal form. To elp h aetna review and respond to your request,. These changes do not affect member appeals. Ask for coverage of a medical service or.
To Elp H Aetna Review And Respond To Your Request,.
Standard appeal if your appeal is about coverage for a medical item or service you have not yet received, you. Web requesting an appeal (redetermination) if you disagree with medicare’s coverage or payment decision. Web have 60 calendar days from the date of your denial to ask us for an appeal. Web provider appeals dispute & appeal process:
Signnow Combines Ease Of Use, Affordability And Security In.
Web you may use this form to appeal multiple dates of service for the same member. Web request for an appeal of an aetna medicare advantage (part c) plan authorization denial. Call us at the number on your member id card, or learn. Because aetna medicare (or one of our delegates) denied your request for.
Web There Are Two Kinds Of Medicare Member Authorization Appeals.
Because aetna medicare (or one of our delegates) denied your request for payment of. Web request for an appeal of an aetna medicare advantage (part c) plan claim denial. Box 7773 london, ky 40742 you may also ask. Exceptions apply to members covered under.
(This Information May Be Found On The Front Of The Member’s Id Card.) Today’s Date Member’s Id Number Plan Type Member’s Group.
In some cases, we may allow exceptions for a. If you are acting on the member’s behalf and have a signed authorization from the member. Web please provide the following information. Aetna medicare appeals po box 14067.