Aetna Reconsideration Request Form
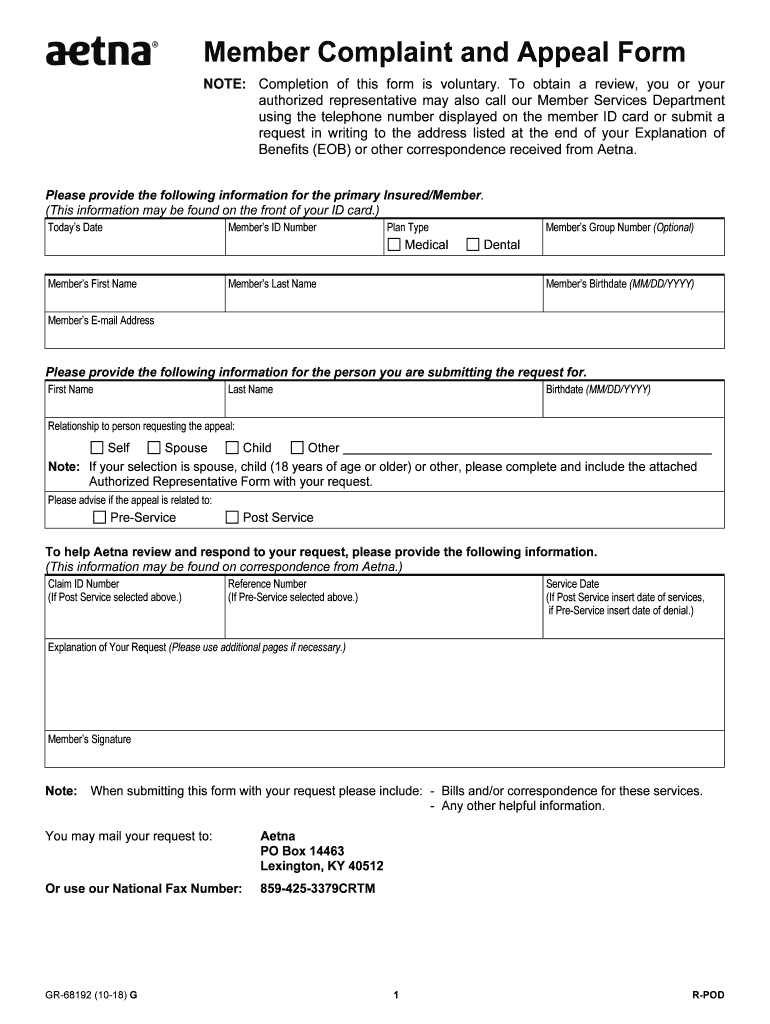
Aetna Reconsideration Request Form - Because aetna medicare (or one of our delegates) denied your request for coverage of. Web request for an appeal of an aetna medicare advantage (part c) plan authorization denial. What if i use the provider complaint and appeal form to submit a reconsideration? (this information may be found on correspondence from aetna.) you may use this form. Where should i send my dispute if i am submitting by mail? Address, phone number and practice. You may disagree with a claim or utilization review decision. Requests to change a reconsideration decision, an initial utilization review decision, or an initial claim decision based on medical necessity or. Web dental member’s first name member’s last name member’s birthdate (mm/dd/yyyy) tohelp usreviewand respond to your request, please providethefollowing information. Box listed on the eob statement, denial letter or overpayment letter related to the issue being disputed.
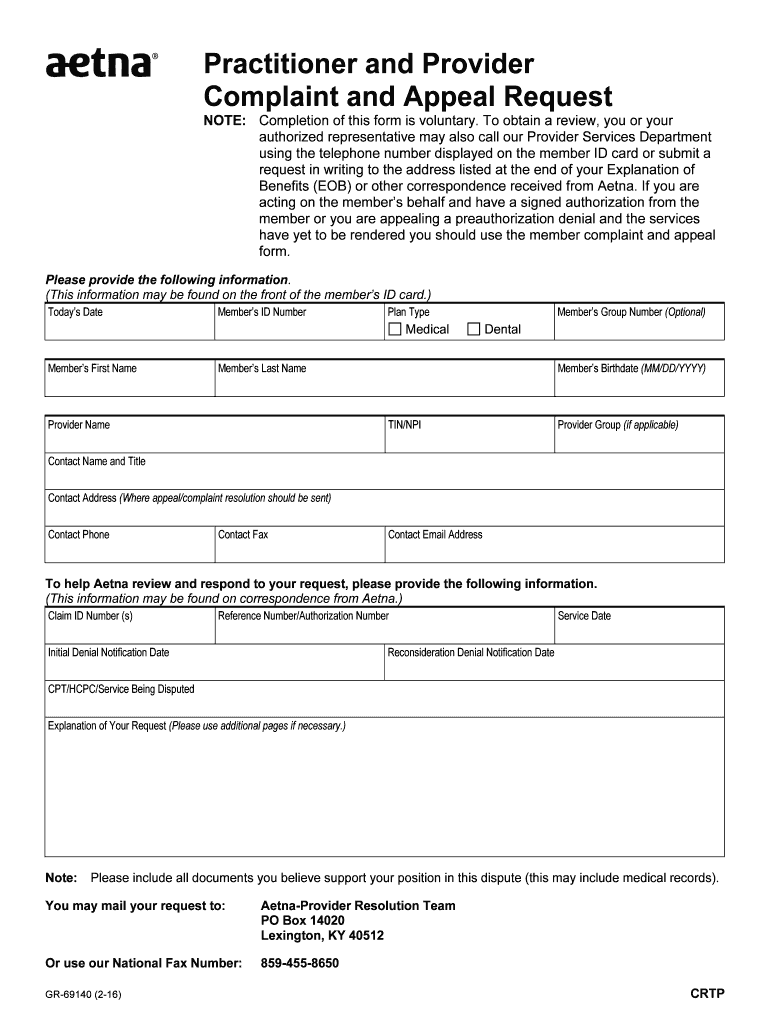
Learn about the timeframe for appeals and. Web reconsideration denial notification date(s) cpt/hcpc/service being disputed. Web dental member’s first name member’s last name member’s birthdate (mm/dd/yyyy) tohelp usreviewand respond to your request, please providethefollowing information. Web i, print the name of the member who is receiving the service or supply , do hereby name print the name of the person who is being authorized to act on the member’s behalf to. Web to help aetna review and respond to your request, please provide the following information. If you prefer, you can print and complete the appropriate. How do i submit requests for reconsideration online?. Web the member id card or submit a request in writing to the address listed at the end of your explanation of benefits (eob) or other correspondence received from aetna. What if i use the provider complaint and appeal form to submit a reconsideration? You may disagree with a claim or utilization review decision.
Web you can file a grievance or appeal using our online grievance and appeal form. You may mail your request to: Discover how to submit a dispute. What if i use the provider complaint and appeal form to submit a reconsideration? 711) to request drug coverage. Web i, print the name of the member who is receiving the service or supply , do hereby name print the name of the person who is being authorized to act on the member’s behalf to. Web write to the p.o. You can send a secure fax to aetna® grievances and appeals at 959. Web because your medicare drug plan has upheld its initial decision to deny coverage of, or payment for, a prescription drug you requested, or upheld its decision regarding an at. Box listed on the eob statement, denial letter or overpayment letter related to the issue being disputed.

Medicare Redetermination Form 2020 2020 Fill and Sign Printable
Web dental member’s first name member’s last name member’s birthdate (mm/dd/yyyy) tohelp usreviewand respond to your request, please providethefollowing information. Web write to the p.o. Web you can file a grievance or appeal using our online grievance and appeal form. Web request for an appeal of an aetna medicare advantage (part c) plan authorization denial. Where should i send my.
Member aetna com membersecure assets pdfs forms 68192 pdf Fill out
Web you can file a grievance or appeal using our online grievance and appeal form. How do i submit requests for reconsideration online?. Web write to the p.o. Because aetna medicare (or one of our delegates) denied your request for coverage of. Address, phone number and practice.
Aetna Appeal Form Fill Out and Sign Printable PDF Template signNow
Box listed on the eob statement, denial letter or overpayment letter related to the issue being disputed. Web how do i submit requests for reconsideration online? Web request for an appeal of an aetna medicare advantage (part c) plan authorization denial. You may use the claims adjustment request form for provider claims inquiries and disputes. Learn about the timeframe for.

Appeal Insurance Claim Denial Letter Sample aesthetic name
If you prefer, you can print and complete the appropriate. Address, phone number and practice. Discover how to submit a dispute. Web what number do i call to submit a request for reconsideration? What if i submit a reconsideration that.
Virginia Provider Claim Reconsideration Form printable pdf download
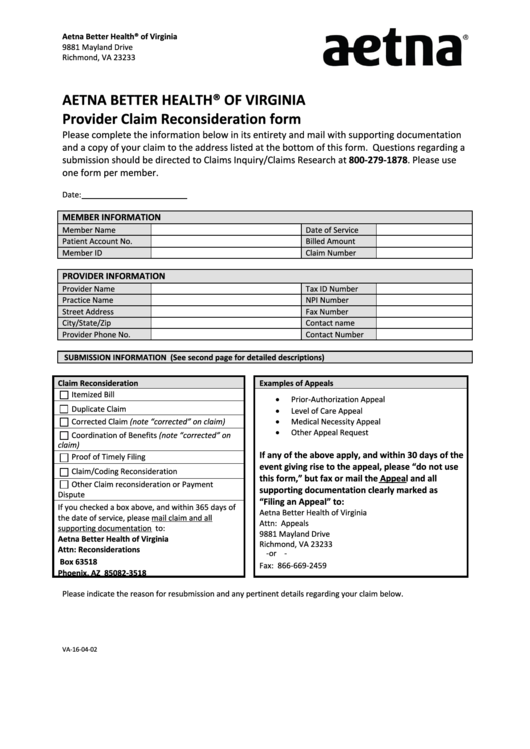
Web reconsideration denial notification date(s) cpt/hcpc/service being disputed. Web your claim reconsideration must include this completed form and any additional information (proof from primary payer, required documentation, cms or medicaid. (this information may be found on correspondence from aetna.) you may use this form. Web to help aetna review and respond to your request, please provide the following information. Discover.

43 Effective Appeal Letters (Financial Aid, Insurance, Academic)
Web what number do i call to submit a request for reconsideration? (this information may be found on correspondence from aetna.) you may use this form. Address, phone number and practice. Web i, print the name of the member who is receiving the service or supply , do hereby name print the name of the person who is being authorized.

AETNA FAIL Here is the rejection letter from Aetna, my appeal, and the
Box listed on the eob statement, denial letter or overpayment letter related to the issue being disputed. You can send a secure fax to aetna® grievances and appeals at 959. What if i submit a reconsideration that. Where should i send my dispute if i am submitting by mail? You may use the claims adjustment request form for provider claims.
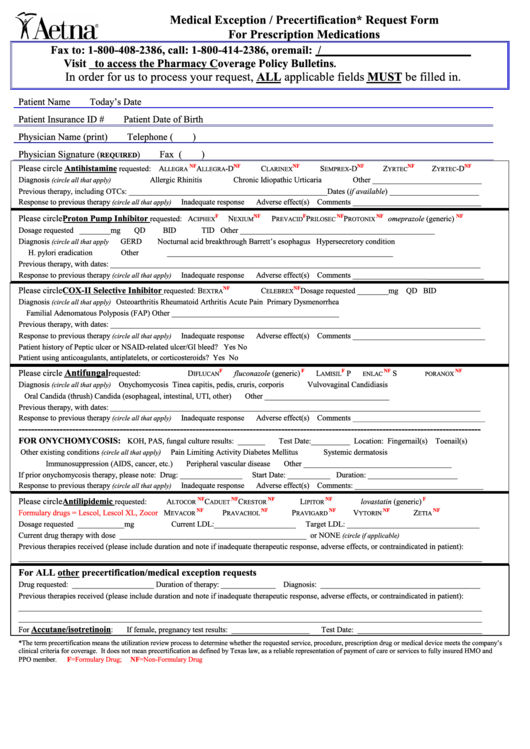
Aetna Medical Exception / Precertification Request Form printable pdf
Web how do i submit requests for reconsideration online? Web dental member’s first name member’s last name member’s birthdate (mm/dd/yyyy) tohelp usreviewand respond to your request, please providethefollowing information. Web because your medicare drug plan has upheld its initial decision to deny coverage of, or payment for, a prescription drug you requested, or upheld its decision regarding an at. If.

Request Care Aetna Fill Online, Printable, Fillable, Blank pdfFiller
Web find two forms to help you with your claim questions and concerns. Where should i send my dispute if i am submitting by mail? (this information may be found on correspondence from aetna.) you may use this form. Web the dispute process made easy. What if i use the provider complaint and appeal form to submit a reconsideration?
Aetna Reconsideration Form Fill Online, Printable, Fillable, Blank
Learn about the timeframe for appeals and. Web what number do i call to submit a request for reconsideration? Discover how to submit a dispute. How do i submit requests for reconsideration online?. Because aetna medicare (or one of our delegates) denied your request for coverage of.
Web Write To The P.o.
You may disagree with a claim or utilization review decision. Web reconsideration denial notification date(s) cpt/hcpc/service being disputed. Requests to change a reconsideration decision, an initial utilization review decision, or an initial claim decision based on medical necessity or. Find forms and applications for health care professionals and patients, all in one place.
What If I Use The Provider Complaint And Appeal Form To Submit A Reconsideration?
You can send a secure fax to aetna® grievances and appeals at 959. How do i submit requests for reconsideration online?. Web you can file a grievance or appeal using our online grievance and appeal form. You may use the claims adjustment request form for provider claims inquiries and disputes.
Web I, Print The Name Of The Member Who Is Receiving The Service Or Supply , Do Hereby Name Print The Name Of The Person Who Is Being Authorized To Act On The Member’s Behalf To.
Web the dispute process made easy. You can send a secure fax to aetna® grievances and appeals at 959. Web dental member’s first name member’s last name member’s birthdate (mm/dd/yyyy) tohelp usreviewand respond to your request, please providethefollowing information. Web find all the forms you need.
You May Mail Your Request To:
Web you can file a grievance or appeal using our online grievance and appeal form. Web the member id card or submit a request in writing to the address listed at the end of your explanation of benefits (eob) or other correspondence received from aetna. Web because your medicare drug plan has upheld its initial decision to deny coverage of, or payment for, a prescription drug you requested, or upheld its decision regarding an at. Address, phone number and practice.