Bcbs Tier Exception Form
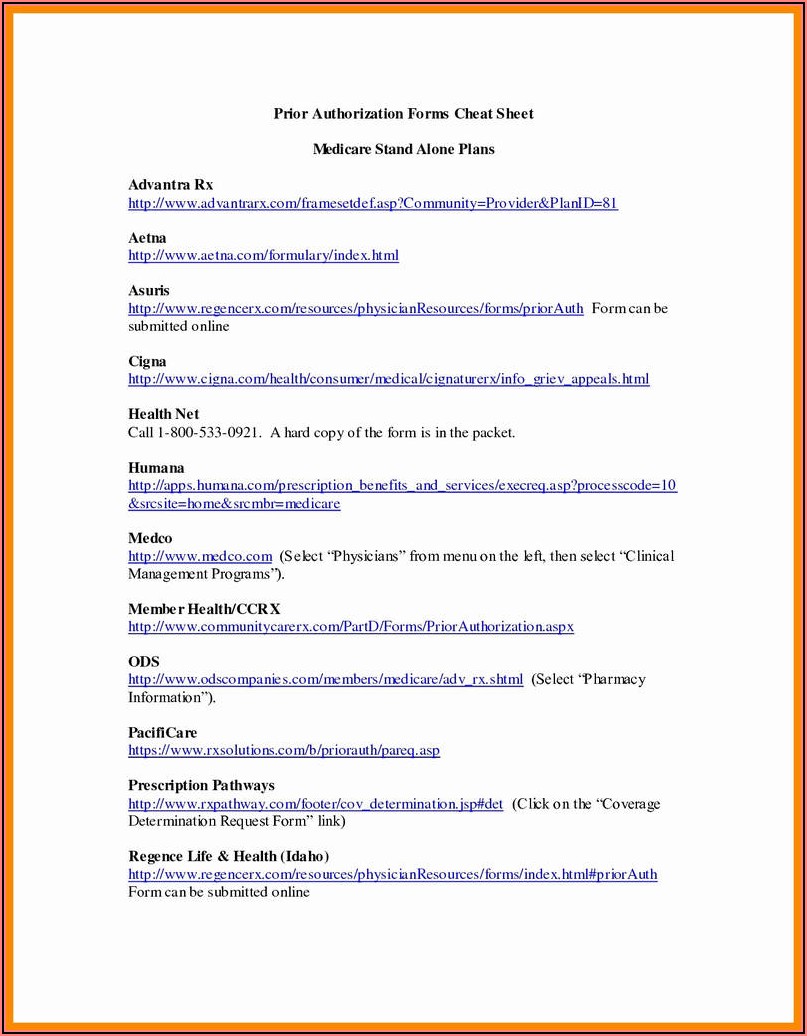
Bcbs Tier Exception Form - Access medicare forms, including claim and enrollment forms, along with plan documents, including provider directories, benefits. (2) explain medical reason] o. Web prescription drug coverage determination form. (1) formulary or preferred drug(s) tried and results of drug. Web please fax this completed form to clinical pharmacy at. Web tier exception (pdf, 109 kb) to submit a request for review for part d drugs unrelated to hospice, use the form below: Web to request coverage of a medication that's not on the plan formulary (list of covered drugs), you can ask for a formulary exception. (1) dosage form(s) and/or dosage(s) tried; Web you and your doctor can submit an exception request for drug coverage. Web tier exception to submit request electronically, please go to covermymeds.com using plan/pbm name “bcbs nc” tier exception request form.
(2) explain medical reason] o. Web please complete the attached request for a lower copay* (tier exception form) to prevent delays in the review process please complete all requested fields. Web tier exception to submit request electronically, please go to covermymeds.com using plan/pbm name “bcbs nc” tier exception request form. Web coordination of benefits/blue cross and blue shield of alabama is host plan; Web need medicare forms or documents? Web tier exception (pdf, 109 kb) to submit a request for review for part d drugs unrelated to hospice, use the form below: If we agree to make an exception and cover a. For your convenience, we've put these commonly used documents together in one place. Web medical need for different dosage form and/or higher dosage [specify below: Web request for formulary tier exception [specify below:
(1) formulary or preferred drugs contraindicated or tried and failed, or tried and not as effective as. ____ / ____ / ______. (1) formulary or preferred drug(s) tried and results of drug. Start by choosing your patient's network listed below. Web > secureblue (hmo) formulary exception and tier request form. Web medical need for different dosage form and/or higher dosage [specify below: Web you and your doctor can submit an exception request for drug coverage. Hospice form (pdf, 123 kb) phone:. Web tier exception (pdf, 109 kb) to submit a request for review for part d drugs unrelated to hospice, use the form below: If you're looking for us to cover a drug that's not currently on our list, you should request a coverage determination.
Top 64 Blue Cross Blue Shield Claim Form Templates free to download in
If we agree to make an exception and cover a. Web request for formulary tier exception [specify below: (1) formulary or preferred drugs contraindicated or tried and failed, or tried and not as effective as. (2) explain medical reason] o. Web to request coverage of a medication that's not on the plan formulary (list of covered drugs), you can ask.
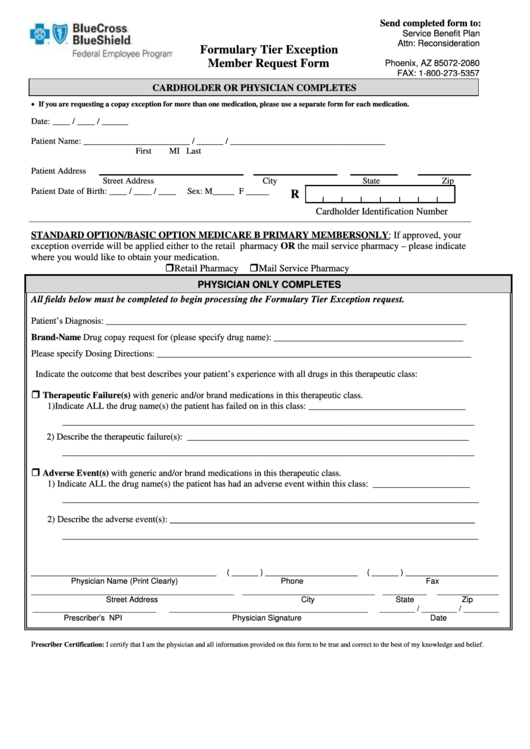
Formulary Tier Exception Member Request Form Service Benefit Plan
Web please complete the attached request for a lower copay* (tier exception form) to prevent delays in the review process please complete all requested fields. Web please fax this completed form to clinical pharmacy at. If we agree to make an exception and cover a. Access medicare forms, including claim and enrollment forms, along with plan documents, including provider directories,.
Optumrx Medicare Part D Tier Exception Form Form Resume Examples
If we agree to make an exception and cover a. If we agree to make an exception and cover a. ____ / ____ / ______. Web ˜ request for formulary tier exception specify below: Web please complete the attached request for a lower copay* (tier exception form) to prevent delays in the review process please complete all requested fields.
Blue Exception Tier Form Fill Online, Printable, Fillable, Blank
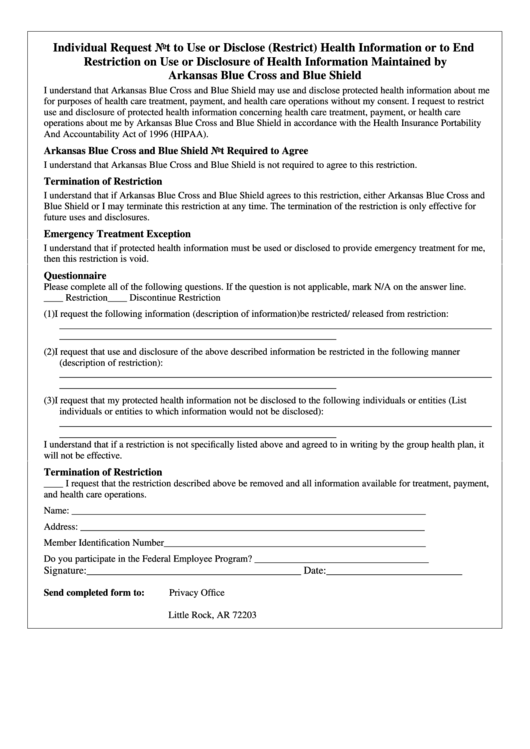
Web tier exception request form (incomplete form may delay processing) please return completed form to: (1) dosage form(s) and/or dosage(s) tried; Web tier exception (pdf, 109 kb) to submit a request for review for part d drugs unrelated to hospice, use the form below: Hospice form (pdf, 123 kb) phone:. Web please fax this completed form to clinical pharmacy at.

ads/responsive.txt Aetna Medicare Tier Exception form Awesome Cigna
Web tier exception to submit request electronically, please go to covermymeds.com using plan/pbm name “bcbs nc” tier exception request form. Web tier exception request form (incomplete form may delay processing) please return completed form to: (2) explain medical reason] o. If we agree to make an exception and cover a. Web please fax this completed form to clinical pharmacy at.

Aetna Medicare Tier Exception form Elegant Aco
Web please fax this completed form to clinical pharmacy at. Web > secureblue (hmo) formulary exception and tier request form. If we agree to make an exception and cover a. Web request for formulary tier exception [specify below: For your convenience, we've put these commonly used documents together in one place.
Texas Bcbs Provider Appeal Fill Out and Sign Printable PDF Template
Web you and your doctor can submit an exception request for drug coverage. Web > secureblue (hmo) formulary exception and tier request form. Web tier exception request form (incomplete form may delay processing) please return completed form to: Web tier exception to submit request electronically, please go to covermymeds.com using plan/pbm name “bcbs nc” tier exception request form. Web request.
OR Regence BCBS Form 5266OR 2018 Fill and Sign Printable Template
Web coordination of benefits/blue cross and blue shield of alabama is host plan; ____ / ____ / ______. Web prescription drug coverage determination form. For your convenience, we've put these commonly used documents together in one place. (1) formulary or preferred drugs contraindicated or tried and failed, or tried and not as effective as.

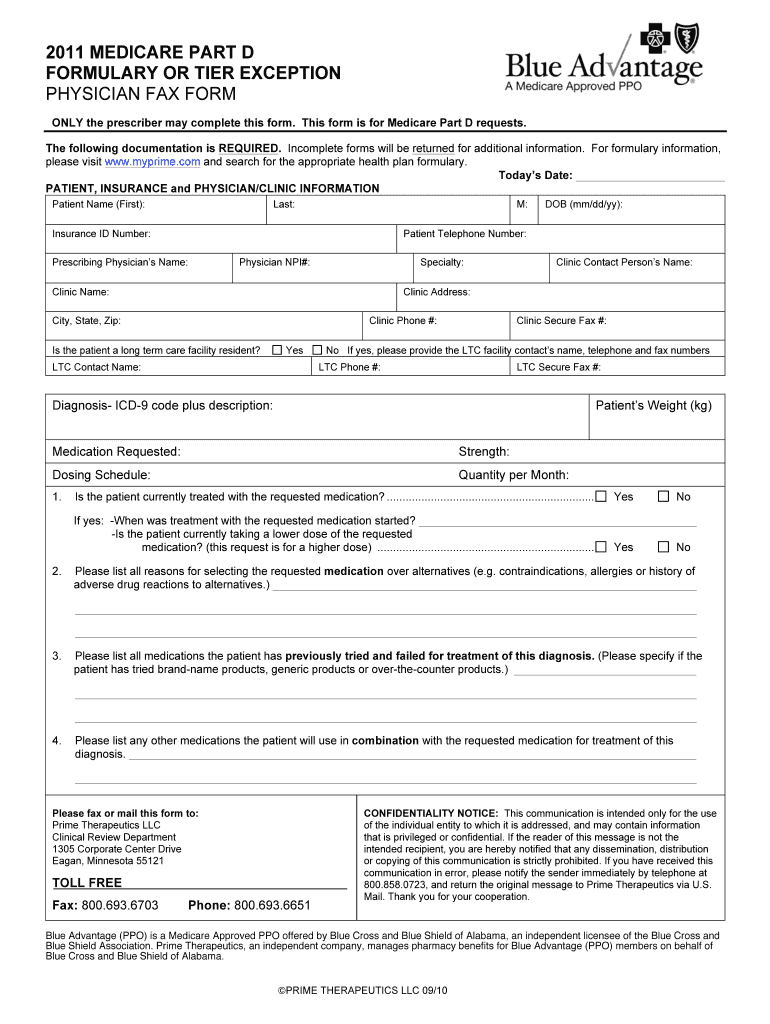
Aarp Medicare Part D Tier Exception Form Form Resume Examples
Web prescription drug coverage redetermination request form (mapd) prescription drug coverage redetermination request form (pdp) prescription drug formulary. Web coordination of benefits/blue cross and blue shield of alabama is host plan; (1) formulary or preferred drugs contraindicated or tried and failed, or tried and not as effective as. If you're looking for us to cover a drug that's not currently.

Gallery of Medicare Tier Exception form Lovely Prescription Drug
Start by choosing your patient's network listed below. Web tier exception to submit request electronically, please go to covermymeds.com using plan/pbm name “bcbs nc” tier exception request form. ____ / ____ / ______. Web request for formulary tier exception [specify below: For your convenience, we've put these commonly used documents together in one place.
Web Prescription Drug Coverage Determination Form.
For your convenience, we've put these commonly used documents together in one place. (1) formulary or preferred drugs contraindicated or tried and failed, or tried and not as effective as. (1) formulary or preferred drugs contraindicated or tried and failed, or tried and not as effective as requested drug; Hospice form (pdf, 123 kb) phone:.
Web Coordination Of Benefits/Blue Cross And Blue Shield Of Alabama Is Host Plan;
Web need medicare forms or documents? If we agree to make an exception and cover a. Web request for formulary tier exception specify below if not noted in the drug history section earlier on the form: If you're looking for us to cover a drug that's not currently on our list, you should request a coverage determination.
Web You And Your Doctor Can Submit An Exception Request For Drug Coverage.
If we agree to make an exception and cover a. Web to request coverage of a medication that's not on the plan formulary (list of covered drugs), you can ask for a formulary exception. ____ / ____ / ______. Web tier exception to submit request electronically, please go to covermymeds.com using plan/pbm name “bcbs nc” tier exception request form.
Web > Secureblue (Hmo) Formulary Exception And Tier Request Form.
Web to request coverage of a medication that's not on the plan formulary (list of covered drugs), you can ask for a formulary exception. Web please fax this completed form to clinical pharmacy at. Web prescription drug coverage redetermination request form (mapd) prescription drug coverage redetermination request form (pdp) prescription drug formulary. (2) explain medical reason] o.