Cms 1500 Form Fields
Cms 1500 Form Fields - It is the basic paper claim form. Web cms 1500 claim form instructions tool. This form is the only version. Web cms 1500 form: Enter the date of service on the top right corner of the form. License for use of physicians' current procedural. Unless otherwise instructed, enter information in the unshaded area. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Insured’s name (last name, first name, middle initial) 7. Cms 1500 form also known as hcfa 1500 and has 33 blocks.
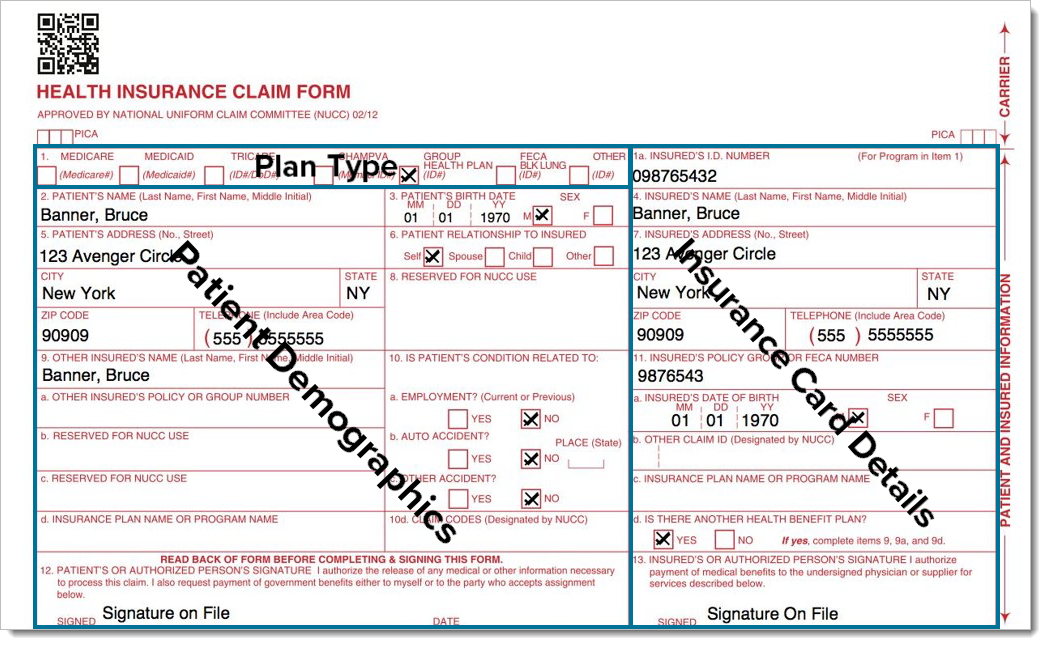
Web cms 1500 form: Insured’s name (last name, first name, middle initial) 7. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Complete, edit or print your forms instantly. The form is used by physicians and allied health professionals to. Access any form you need. License for use of physicians' current procedural. Cms 1500 form also known as hcfa 1500 and has 33 blocks. This form is the only version. Number (for program in item 1) 4.
Consisting of an alternate id or the subscriber's ssn. Cms 1500 form also known as hcfa 1500 and has 33 blocks. This form is the only version. Web cms 1500 form: The form is used by physicians and allied health professionals to. Web up to $40 cash back 1. Number (for program in item 1) 4. Web cms 1500 dynamic list information. Fill out the health insurance claim form online and print it out for free. Ad download or email cms 1500 & more fillable forms, register and subscribe now!
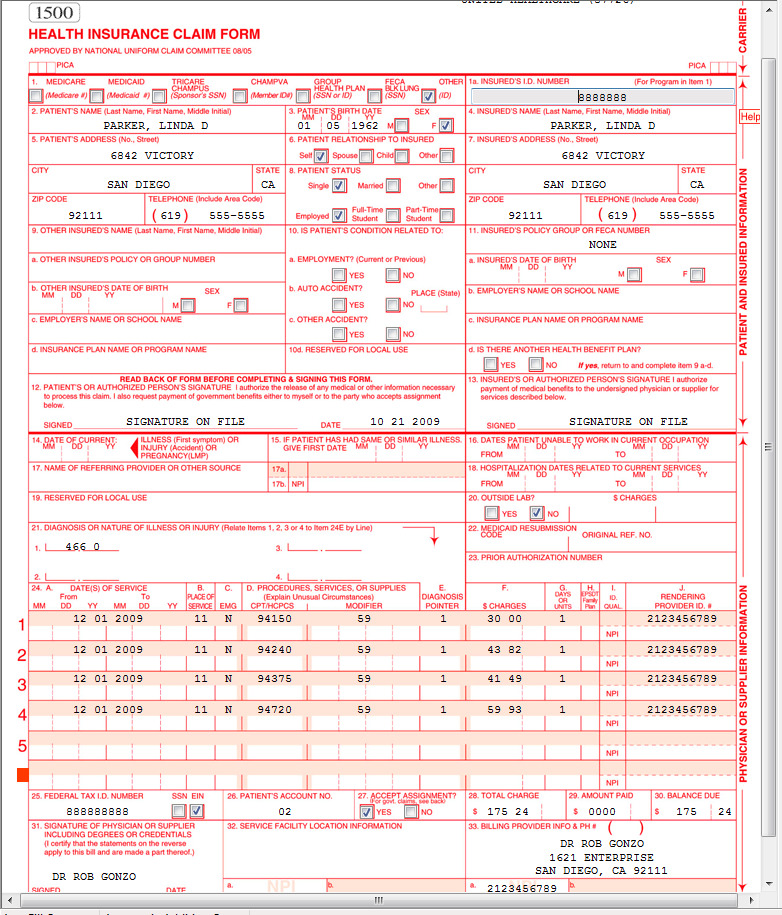
cms1500claimformsample CASO Document Management
The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Number (for program in item 1) 4. The 837p (professional) is the standard format used by health care professionals and suppliers to transmit health care claims. Enter the date of service on the top right corner of the form. Download or email cms.
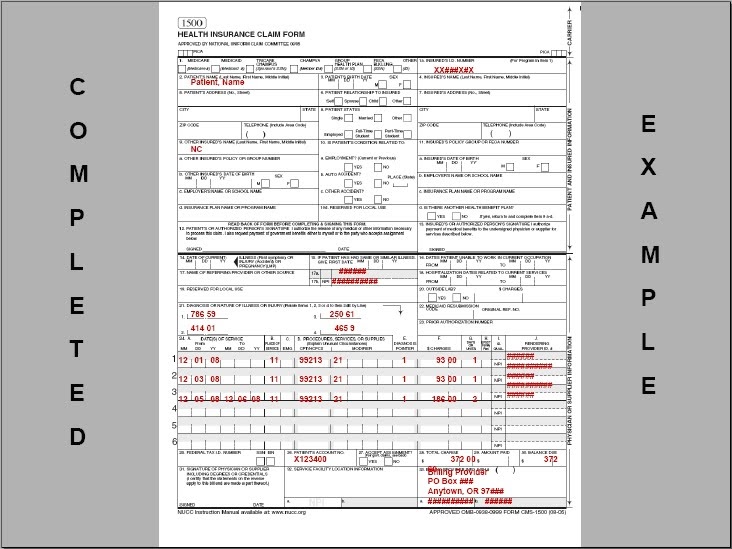
Completed CMS 1500 form CMS 1500 claim form and UB 04 form
This form is the only version. Access any form you need. The 837p (professional) is the standard format used by health care professionals and suppliers to transmit health care claims. Consisting of an alternate id or the subscriber's ssn. Web cms 1500 form:
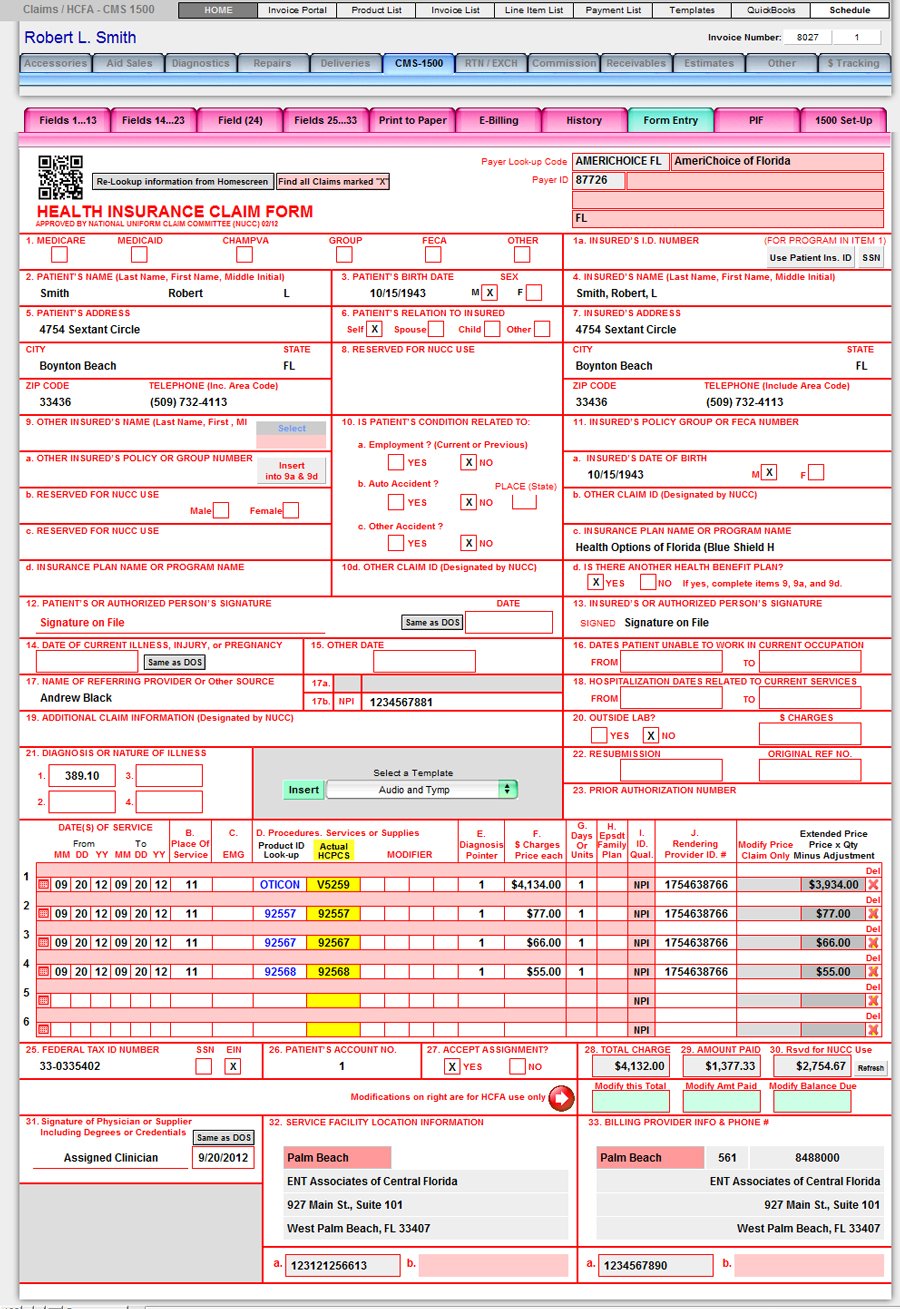
CMS1500 (PQRS Ready) Financial and Billing HearForm Features
Consisting of an alternate id or the subscriber's ssn. Web up to $40 cash back 1. License for use of physicians' current procedural. Web cms 1500 claim form instructions tool. This form is used by providers to submit a claim to the insurance company for the.

Cms 1500 Claim Form Fields Universal Network
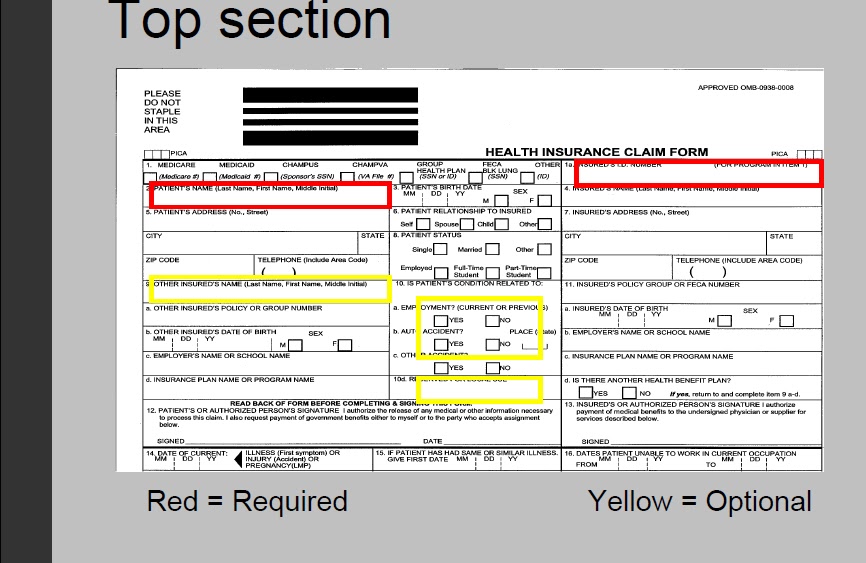
Web up to $40 cash back 1. License for use of physicians' current procedural. Enter the date of service on the top right corner of the form. Web 1500 required fields number and name. Consisting of an alternate id or the subscriber's ssn.
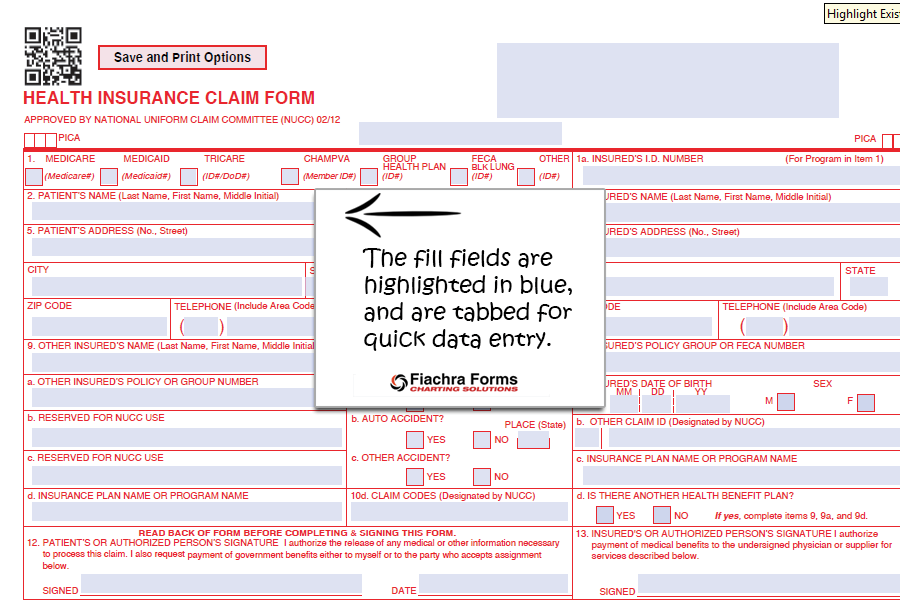
CMS 1500 PDF Template Fiachra Forms Charting Solutions
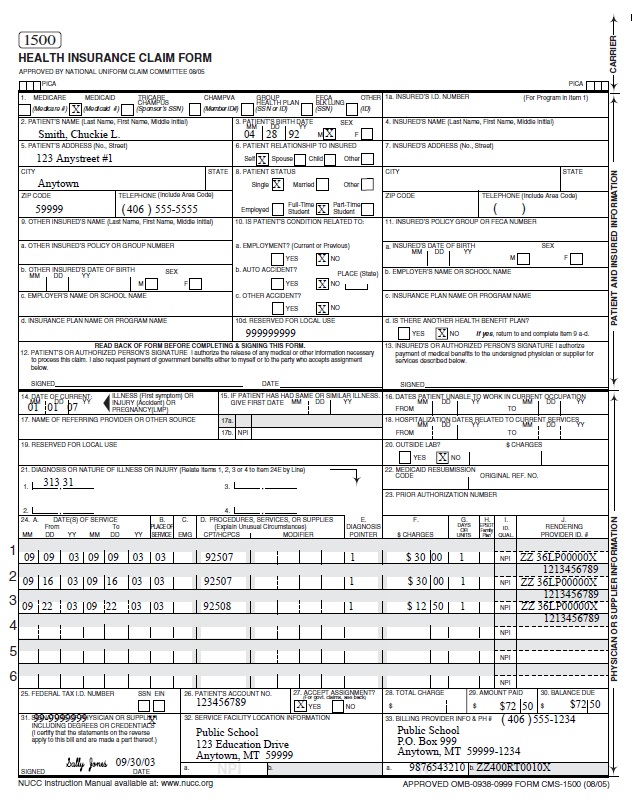
Unless otherwise instructed, enter information in the unshaded area. The form is used by physicians and allied health professionals to. Fill out the health insurance claim form online and print it out for free. This form is used by providers to submit a claim to the insurance company for the. Insured’s name (last name, first name, middle initial) 7.
Medicare PQRI 2007 Provider Call
The form is used by physicians and allied health professionals to. This form is the only version. Complete, edit or print your forms instantly. This form is used by providers to submit a claim to the insurance company for the. Cms 1500 claim form instructions tool.

Cms 1500 Claim Form Pdf Free Download Universal Network
License for use of physicians' current procedural. Ad download or email cms 1500 & more fillable forms, register and subscribe now! Consisting of an alternate id or the subscriber's ssn. Enter the patient's name, address, date of birth, and insurance information in the spaces provided. Web cms 1500 claim form instructions tool.
schoolbasedservicesmanual
Web 1500 required fields number and name. The 837p (professional) is the standard format used by health care professionals and suppliers to transmit health care claims. Consisting of an alternate id or the subscriber's ssn. This form is used by providers to submit a claim to the insurance company for the. Web up to $40 cash back 1.
Paper Claim (CMS1500) Overview Therabill
Cms 1500 claim form instructions tool. Web the center of medicaid and medicare services (cms) form 1500 must be used to bill sfhp for medical services. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Fill out the health insurance claim form online and print it out for free. Enter the date.
CMS 1500 IMAGE TOP section CMS 1500 claim form and UB 04 form
Web cms 1500 claim form instructions tool. The 837p (professional) is the standard format used by health care professionals and suppliers to transmit health care claims. This form is the only version. Ad download or email cms 1500 & more fillable forms, register and subscribe now! Access any form you need.
Access Any Form You Need.
Web apr 20, 2021 knowledge title cms 1500 claim form boxes & corresponding officemate fields (officemate v8.0). Web the center of medicaid and medicare services (cms) form 1500 must be used to bill sfhp for medical services. The 837p (professional) is the standard format used by health care professionals and suppliers to transmit health care claims. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers.
Web Cms 1500 Form:
Download or email cms 1500 & more fillable forms, register and subscribe now! Unless otherwise instructed, enter information in the unshaded area. Ad download or email cms 1500 & more fillable forms, register and subscribe now! Consisting of an alternate id or the subscriber's ssn.
Cms 1500 Claim Form Instructions Tool.
Web cms 1500 dynamic list information. Complete, edit or print your forms instantly. Number (for program in item 1) 4. Insured’s name (last name, first name, middle initial) 7.
Web 1500 Required Fields Number And Name.
License for use of physicians' current procedural. Enter the patient's name, address, date of birth, and insurance information in the spaces provided. This form is used by providers to submit a claim to the insurance company for the. This form is the only version.