Cobra Election Form
Cobra Election Form - Web the consolidated omnibus budget reconciliation act (cobra) health benefit provisions amend the employee retirement income security act, the internal revenue code and the public health service act to require group health plans to provide a temporary continuation of group health coverage that otherwise might be terminated. Your employer or administrator has only 45 days to send you the paperwork. Cobra continuation coverage assistance provides information on continuation health coverage opportunities. Single single single family family family you do not have to send any payment with the election form. Web cobra election form california department of human resources state of california 1. It also requires employers and plans to provide notice. Please use this form only if you're eligible for cobra and only if you've received a cobra election notice in the mail. Web cobra continuation coverage will cost: Web qualified beneficiaries must be given an election period of at least 60 days during which each qualified beneficiary may choose whether to elect cobra coverage. Web cobra outlines how employees and family members may elect continuation coverage.
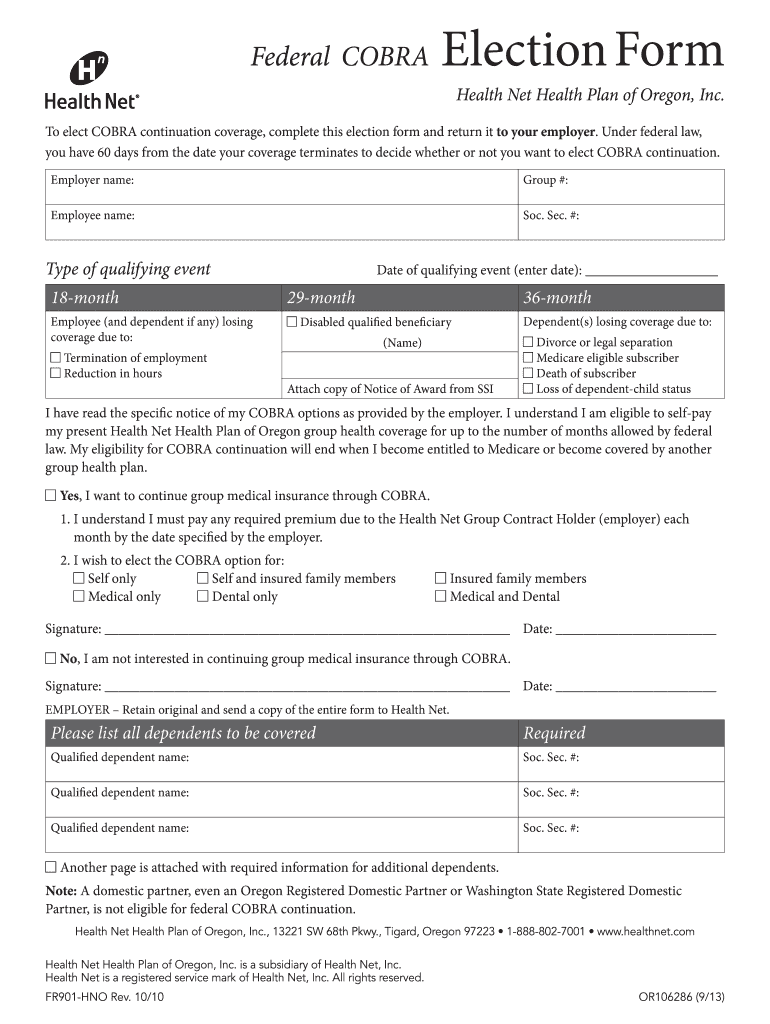
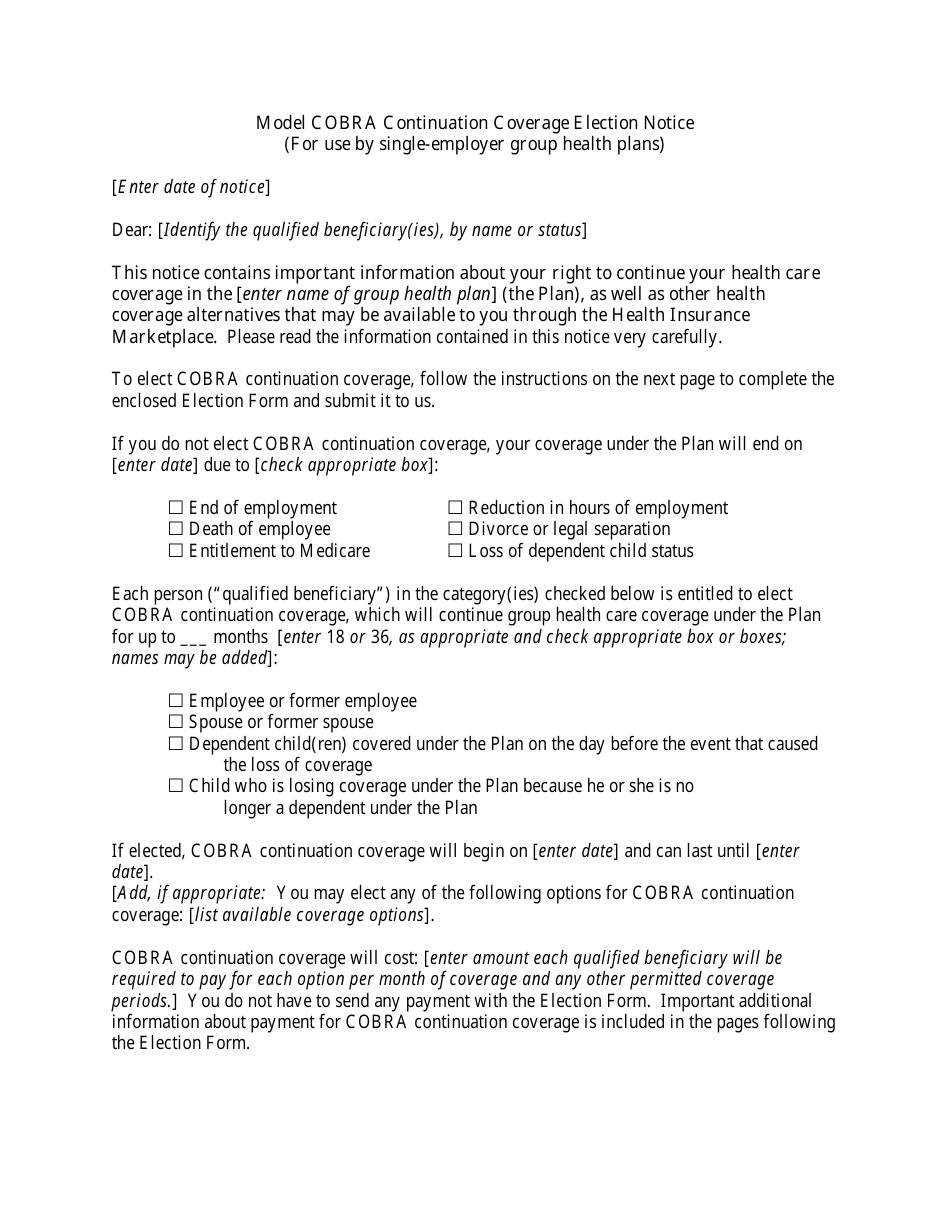
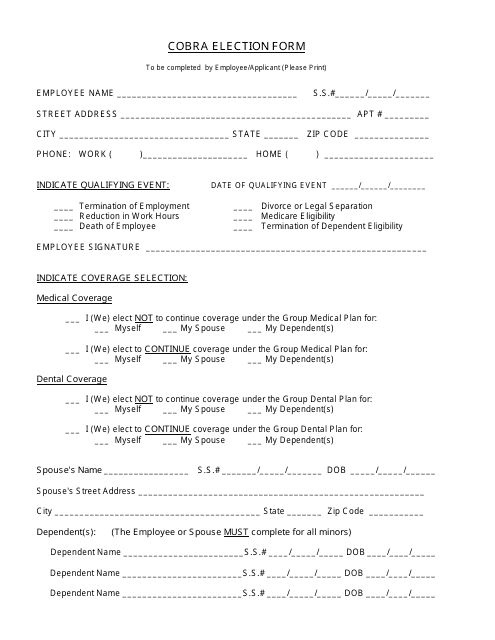
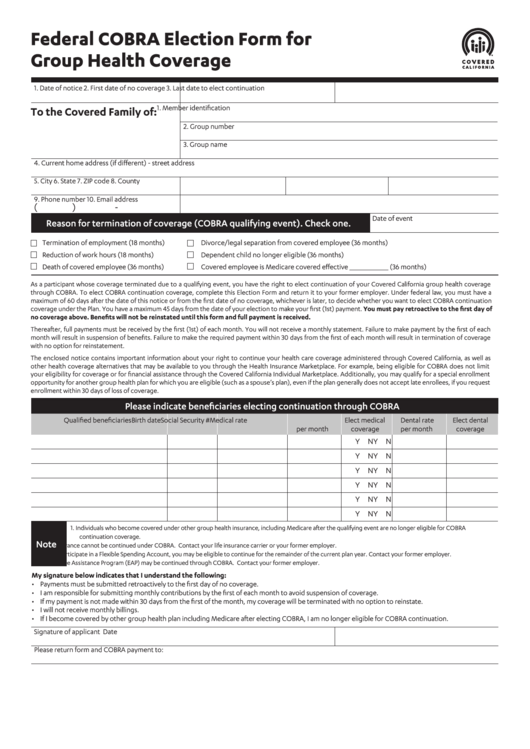
Web cobra continuation coverage will cost: If you don’t submit a completed election form by the due date shown above, you’ll lose your right to elect cobra continuation coverage. Web cobra election form california department of human resources state of california 1. Your employer or administrator has only 45 days to send you the paperwork. Important additional information about payment for cobra continuation coverage is included in the pages following the election form. Web cobra election form complete online use this form to indicate which cobra coverage election(s) you want and for whom you want coverage. Cobra continuation coverage assistance provides information on continuation health coverage opportunities. This period is measured from the later of the date of the qualifying event or the date the cobra election notice is provided. The notice will provide additional details about the cobra premium assistance and how to request it. It also requires employers and plans to provide notice.
Web cobra election form complete online use this form to indicate which cobra coverage election(s) you want and for whom you want coverage. Please use this form only if you're eligible for cobra and only if you've received a cobra election notice in the mail. It also requires employers and plans to provide notice. If you don’t submit a completed election form by the due date shown above, you’ll lose your right to elect cobra continuation coverage. Web cobra election form california department of human resources state of california 1. Cobra continuation coverage assistance provides information on continuation health coverage opportunities. Web cobra continuation coverage will cost: Even if your enrollment is delayed, you will be covered by cobra starting the day your prior coverage ended. Web this election form must be completed and returned by mail [or describe other means of submission and due date]. Web cobra outlines how employees and family members may elect continuation coverage.
New Model COBRA Notice Released MyHRConcierge
If you don’t submit a completed election form by the due date shown above, you’ll lose your right to elect cobra continuation coverage. Even if your enrollment is delayed, you will be covered by cobra starting the day your prior coverage ended. Important additional information about payment for cobra continuation coverage is included in the pages following the election form..
Cobra Form Fill Out and Sign Printable PDF Template signNow
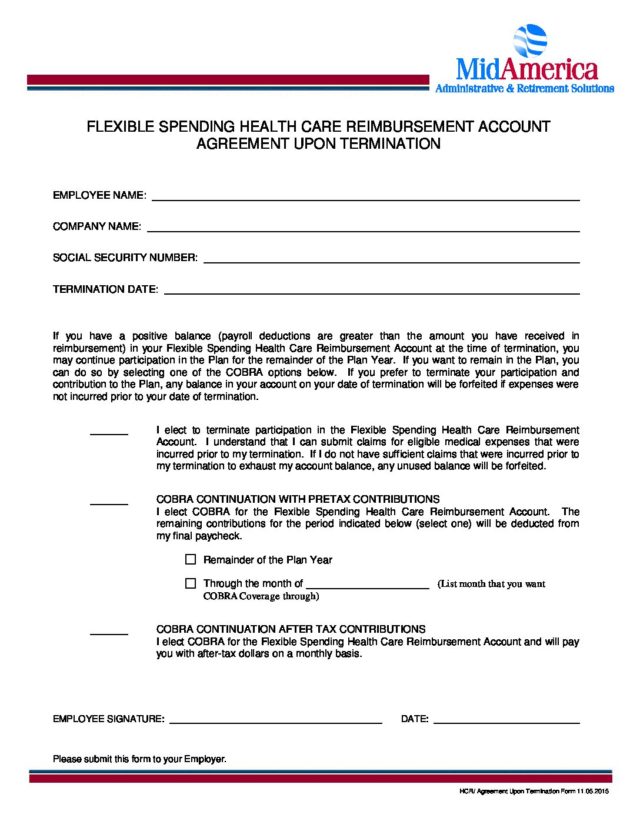
Single single single family family family you do not have to send any payment with the election form. Even if your enrollment is delayed, you will be covered by cobra starting the day your prior coverage ended. The notice will provide additional details about the cobra premium assistance and how to request it. Cobra enrollee information namesocial security number address.
Model Cobra Continuation Coverage Election Notice Form Download
Cobra continuation coverage assistance provides information on continuation health coverage opportunities. Web qualified beneficiaries must be given an election period of at least 60 days during which each qualified beneficiary may choose whether to elect cobra coverage. Single single single family family family you do not have to send any payment with the election form. Cobra enrollee information namesocial security.
COBRA Election Form MidAmerica
Web cobra outlines how employees and family members may elect continuation coverage. Please use this form only if you're eligible for cobra and only if you've received a cobra election notice in the mail. Web cobra continuation coverage will cost: If you don’t submit a completed election form by the due date shown above, you’ll lose your right to elect.
Cobra Election Form Download Printable PDF Templateroller
This period is measured from the later of the date of the qualifying event or the date the cobra election notice is provided. It also requires employers and plans to provide notice. Web qualified beneficiaries must be given an election period of at least 60 days during which each qualified beneficiary may choose whether to elect cobra coverage. The notice.
Cobra Continuation of Coverage Request Template
Please use this form only if you're eligible for cobra and only if you've received a cobra election notice in the mail. Web the consolidated omnibus budget reconciliation act (cobra) health benefit provisions amend the employee retirement income security act, the internal revenue code and the public health service act to require group health plans to provide a temporary continuation.

Form CALHR767 Download Fillable PDF or Fill Online Cobra Election Form
Web cobra election form california department of human resources state of california 1. Even if your enrollment is delayed, you will be covered by cobra starting the day your prior coverage ended. Web this election form must be completed and returned by mail [or describe other means of submission and due date]. It also requires employers and plans to provide.

Offering of Cobra Continuation Coverage Form Fill Out and Sign
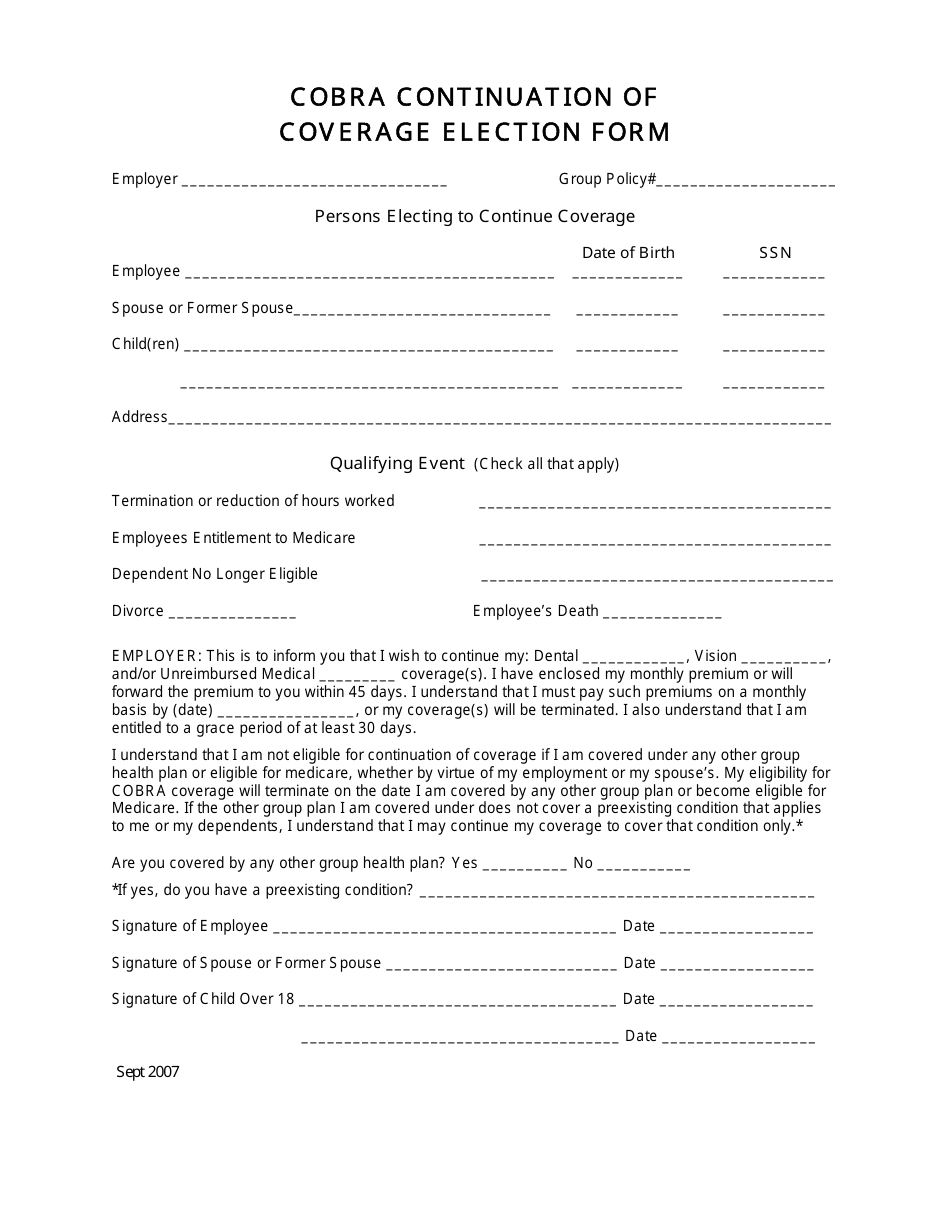
Your employer or administrator has only 45 days to send you the paperwork. Even if your enrollment is delayed, you will be covered by cobra starting the day your prior coverage ended. Web cobra election form complete online use this form to indicate which cobra coverage election(s) you want and for whom you want coverage. It also requires employers and.
Federal Cobra Election Form For Group Health Coverage printable pdf
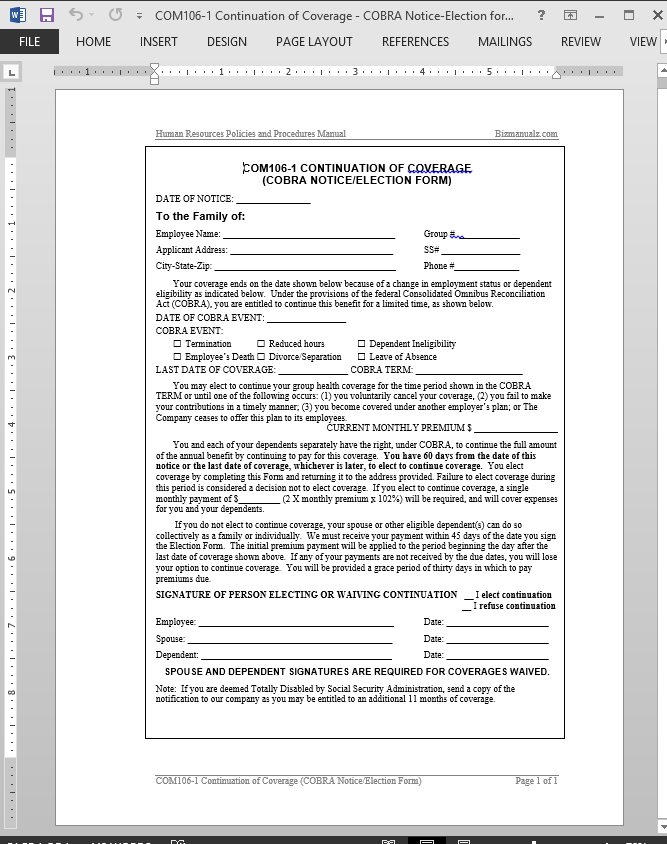
Even if your enrollment is delayed, you will be covered by cobra starting the day your prior coverage ended. This period is measured from the later of the date of the qualifying event or the date the cobra election notice is provided. Web cobra outlines how employees and family members may elect continuation coverage. Web cobra continuation coverage will cost:.
Cobra Continuation of Coverage Election Form Download Printable PDF
Web cobra election form complete online use this form to indicate which cobra coverage election(s) you want and for whom you want coverage. Web cobra outlines how employees and family members may elect continuation coverage. Your employer or administrator has only 45 days to send you the paperwork. Even if your enrollment is delayed, you will be covered by cobra.
Cobra Enrollee Information Namesocial Security Number Address Number And Street City, State, Zip Codephone Number (Optional) If The Enrollee Is Not The Employee, Then Provide The Employee's Name And Social Security Number, And Your Relationship To The.
Web qualified beneficiaries must be given an election period of at least 60 days during which each qualified beneficiary may choose whether to elect cobra coverage. If you don’t submit a completed election form by the due date shown above, you’ll lose your right to elect cobra continuation coverage. Please use this form only if you're eligible for cobra and only if you've received a cobra election notice in the mail. Single single single family family family you do not have to send any payment with the election form.
Your Employer Or Administrator Has Only 45 Days To Send You The Paperwork.
Web cobra continuation coverage will cost: It also requires employers and plans to provide notice. Even if your enrollment is delayed, you will be covered by cobra starting the day your prior coverage ended. Web this election form must be completed and returned by mail [or describe other means of submission and due date].
Important Additional Information About Payment For Cobra Continuation Coverage Is Included In The Pages Following The Election Form.
This period is measured from the later of the date of the qualifying event or the date the cobra election notice is provided. Cobra continuation coverage assistance provides information on continuation health coverage opportunities. Web the consolidated omnibus budget reconciliation act (cobra) health benefit provisions amend the employee retirement income security act, the internal revenue code and the public health service act to require group health plans to provide a temporary continuation of group health coverage that otherwise might be terminated. Web cobra election form complete online use this form to indicate which cobra coverage election(s) you want and for whom you want coverage.
Web Cobra Outlines How Employees And Family Members May Elect Continuation Coverage.
Web cobra election form california department of human resources state of california 1. The notice will provide additional details about the cobra premium assistance and how to request it.