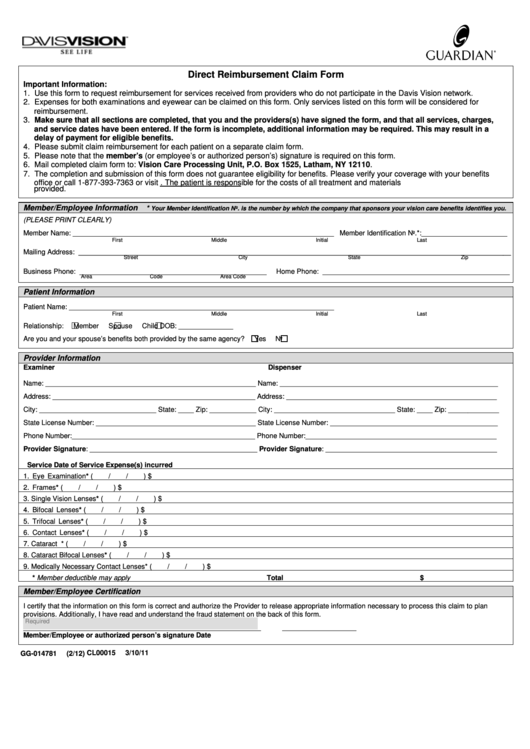
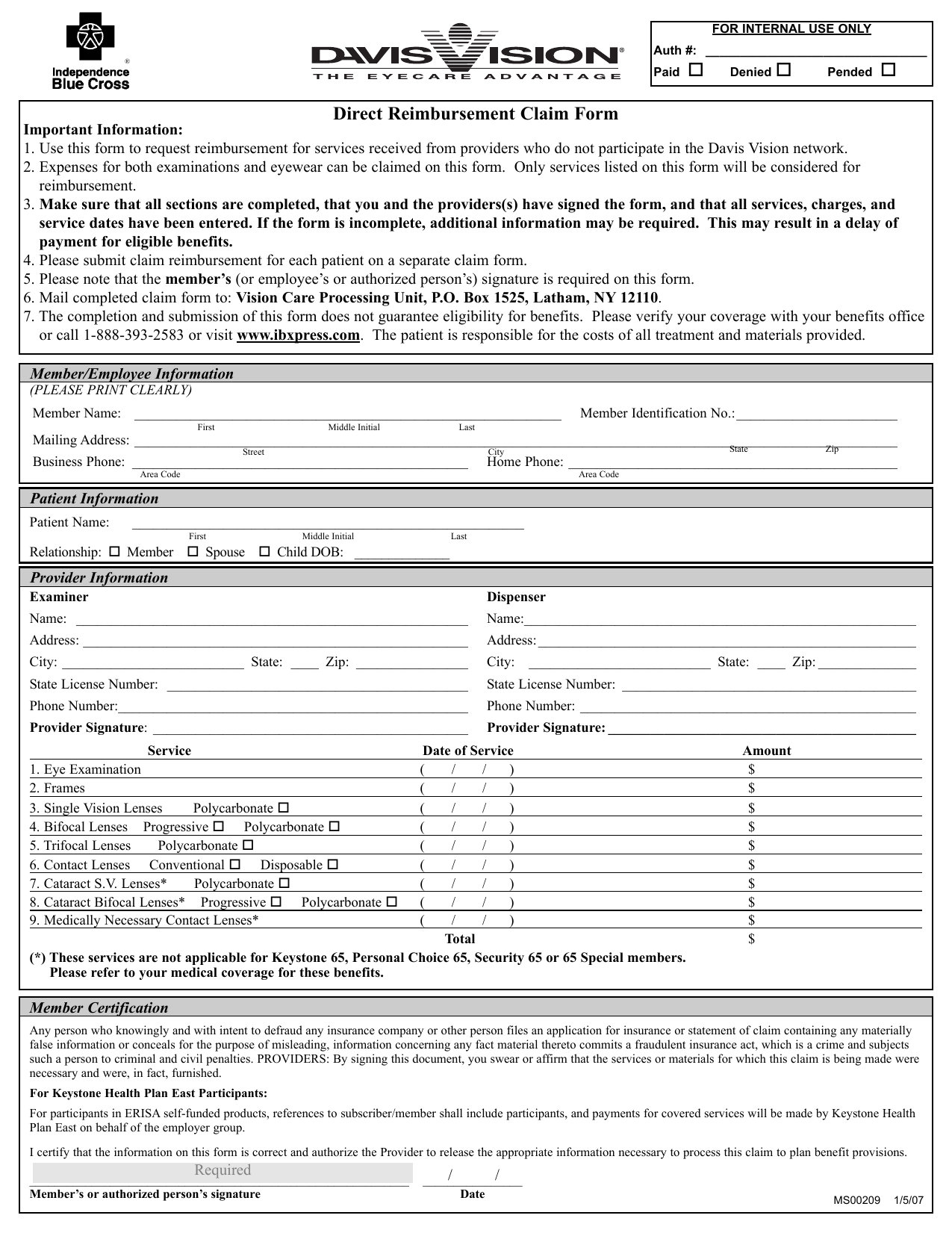
Davis Vision Claim Form
Davis Vision Claim Form - Use this form to request reimbursement for services received from providers who do not participate in the davis vision network. To request reimbursement, complete and print this form, enclose a legible copy of your itemized receipt(s), and send them to the following address. Use this form to request reimbursement for services received from providers not in the davis vision network. Davis vision is a separate company that performs claims administration for your vision program. You must include either your eye care professional’s signature or a detailed receipt. Client / group name the request is regarding; Be sure to keep a copy for your records. Expenses for both examinations and eyewear can be claimed on this form. Expenses for both examinations and eyewear can be claimed on this form. Only services listed on this form will be considered for reimbursement.
Follow the instructions on the form to submit your claim. Client / group name the request is regarding; To request reimbursement, complete and print this form, enclose a legible copy of your itemized receipt(s), and send them to the following address. Use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Box 791 latham, ny 12110 fax: (choose one) ☐member ☐spouse ☐domestic partner. Be sure that all sections have been completed and that you and the provider(s) have. Use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Expenses for both examinations and eyewear can be claimed on this form.
Web davis vision has been providing comprehensive vision care benefits for over 50 years. Each patient’s services must be claimed on a separate form. Use this form to request reimbursement for services received from providers not in the davis vision network. Letter of authorization from client / group; Web log in to your account and click on “access benefits and forms” to download the direct reimbursement claim form. Only services listed on this form will be considered for reimbursement. If a corrected claim has been attached, please specify revisions that were made: Be sure to keep a copy for your records. Use this form to request reimbursement for services received from providers who do not participate in the davis vision network. This change aligns davis vision and superior vision with cms guidelines on paper claims submission.

Say Hello to the Brandnew Davis Vision Mobile App TeamstersCare 25
Web direct reimbursement claim form important information: Client / group name the request is regarding; Use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Web direct reimbursement claim form.
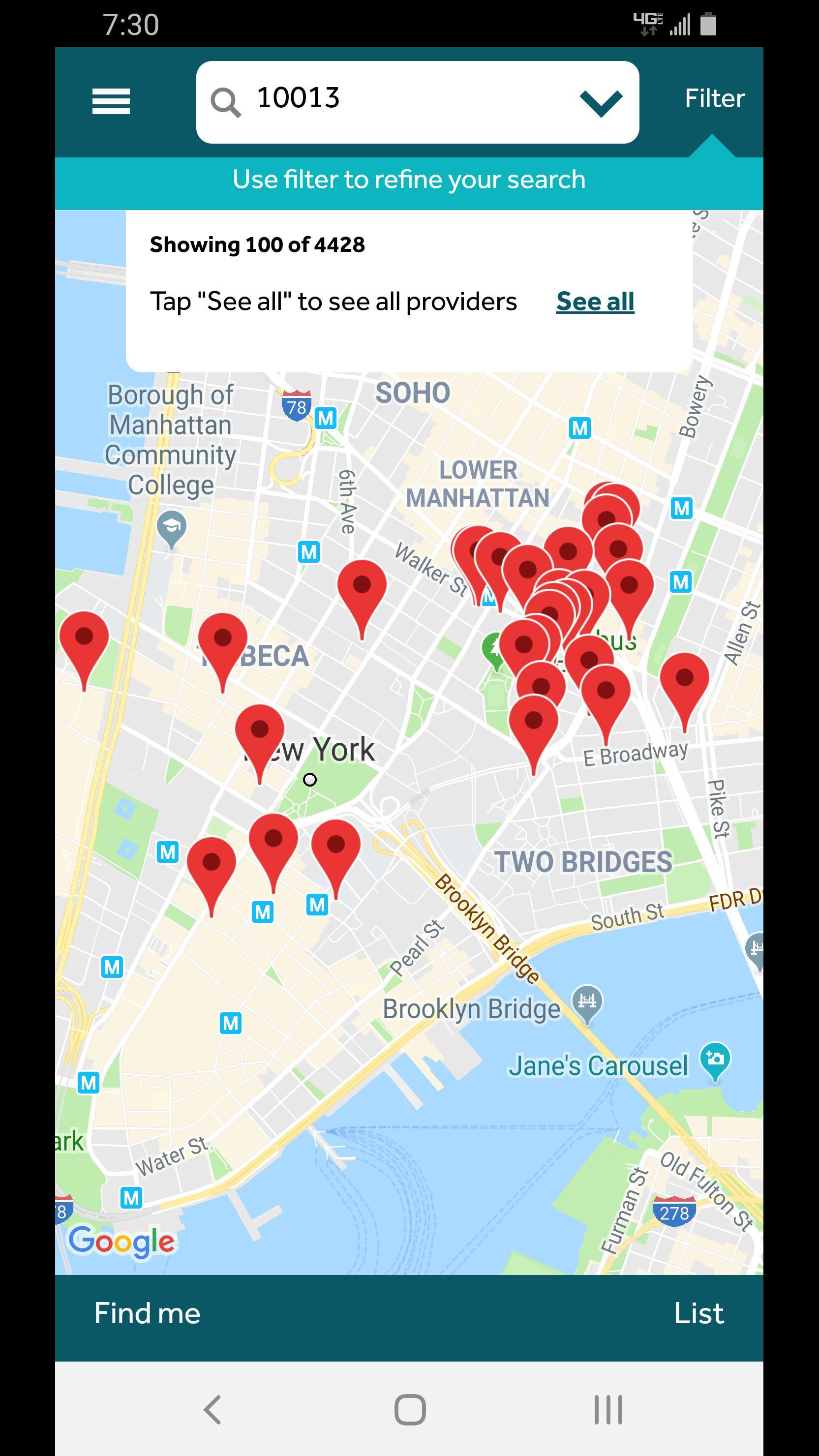
Davis Vision for Android APK Download
Use this form to request reimbursement for services received from providers who do not participate in the davis vision network. Only services listed on this form will be considered for reimbursement. Client / group name the request is regarding; Follow the instructions on the form to submit your claim. Use this form to request reimbursement for services received from providers.

Davis Vision Insurance Providers Near Me Vision Care Plans Plans We
Expenses for both examinations and eyewear can be claimed on this form. You must include either your eye care professional’s signature or a detailed receipt. Be sure to keep a copy for your records. Web davis vision by metlife member reimbursement form. Only services listed on this form will be considered for reimbursement.
Top Davis Vision Claim Form Templates Free To Download In PDF Format
Be sure that all sections have been completed and that you and the provider(s) have. To request reimbursement, complete and print this form, enclose a legible copy of your itemized receipt(s), and send them to the following address. Web direct reimbursement claim form important information: Letter of authorization from client / group; Expenses for both examinations and eyewear can be.

Davis Vision "Out of Network" claim form by Drs. Stahl & Calder Issuu
Expenses for both examinations and eyewear can be claimed on this form. Davis vision is a separate company that performs claims administration for your vision program. Client / group name the request is regarding; Please submit to the following contact: Web davis vision has been providing comprehensive vision care benefits for over 50 years.

Claim Form Davis Vision Claim Form
Follow the instructions on the form to submit your claim. This change aligns davis vision and superior vision with cms guidelines on paper claims submission. Expenses for both examinations and eyewear can be claimed on this form. To request reimbursement, complete and print this form, enclose a legible copy of your itemized receipt(s), and send them to the following address..
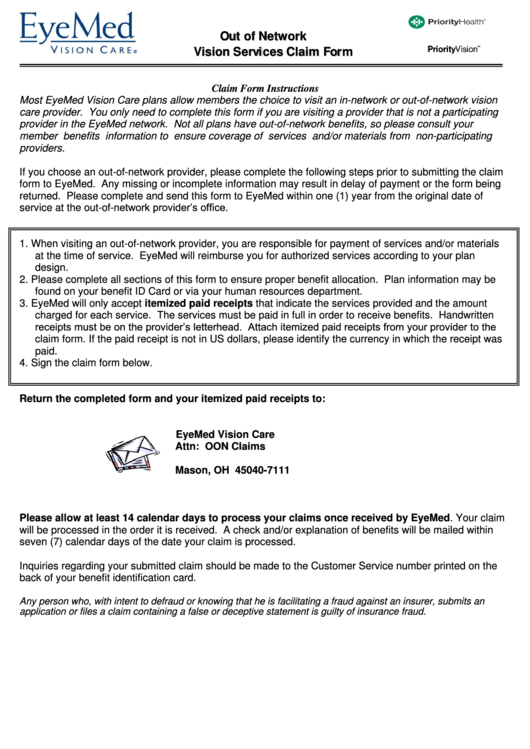
Vision Services Claim Form 2012 printable pdf download
Please submit to the following contact: Box 791 latham, ny 12110 fax: Expenses for both examinations and eyewear can be claimed on this form. Only services listed on this form will be considered for reimbursement. Be sure to keep a copy for your records.

Always Care Vision Claim Form 20202021 Fill and Sign Printable
Only services listed on this form will be considered for reimbursement. Letter of authorization from client / group; Be sure to keep a copy for your records. Davis vision complaints and appeals department p.o. Use this form to request reimbursement for services received from providers who do not participate in the davis vision network.
Download Davis Vision Claim Form PDF
If a corrected claim has been attached, please specify revisions that were made: Client / group name the request is regarding; Web direct reimbursement claim form important information: Box 791 latham, ny 12110 fax: Use this form to request reimbursement for services received from providers who do not participate in the davis vision network.

Davis Vision's integration strategy criticized in lawsuit and
To request reimbursement, complete and print this form, enclose a legible copy of your itemized receipt(s), and send them to the following address. This change aligns davis vision and superior vision with cms guidelines on paper claims submission. (choose one) ☐member ☐spouse ☐domestic partner. Only services listed on this form will be considered for reimbursement. Web log in to your.
Web Direct Reimbursement Claim Form Important Information:
Please submit to the following contact: Client / group name the request is regarding; Web davis vision by metlife member reimbursement form. Each patient’s services must be claimed on a separate form.
Web Vendor Maintenance Request Form (Excel) Additionally, Ensure You Include The Following:
Expenses for both examinations and eyewear can be claimed on this form. Only services listed on this form will be considered for reimbursement. Web direct reimbursement claim form important information: (choose one) ☐member ☐spouse ☐domestic partner.
Use This Form To Request Reimbursement For Services Received From Providers Who Do Not Participate In The Davis Vision Network.
If a corrected claim has been attached, please specify revisions that were made: Use this form to request reimbursement for services received from providers who do not participate in the davis vision network. To request reimbursement, complete and print this form, enclose a legible copy of your itemized receipt(s), and send them to the following address. Box 791 latham, ny 12110 fax:
Letter Of Authorization From Client / Group;
Be sure that all sections have been completed and that you and the provider(s) have. Expenses for both examinations and eyewear can be claimed on this form. Expenses for both examinations and eyewear can be claimed on this form. Davis vision complaints and appeals department p.o.