Hcfa 1500 Form Printable
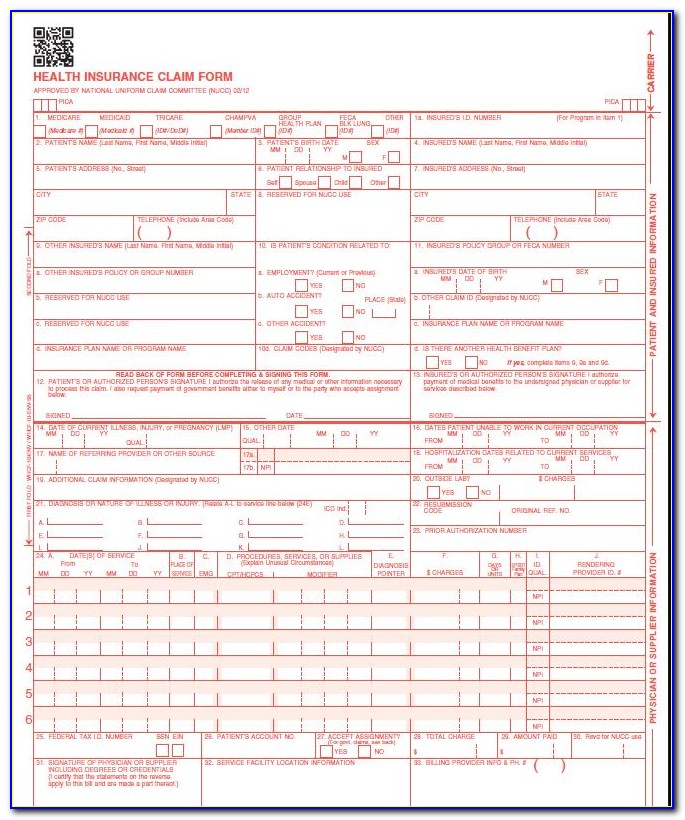
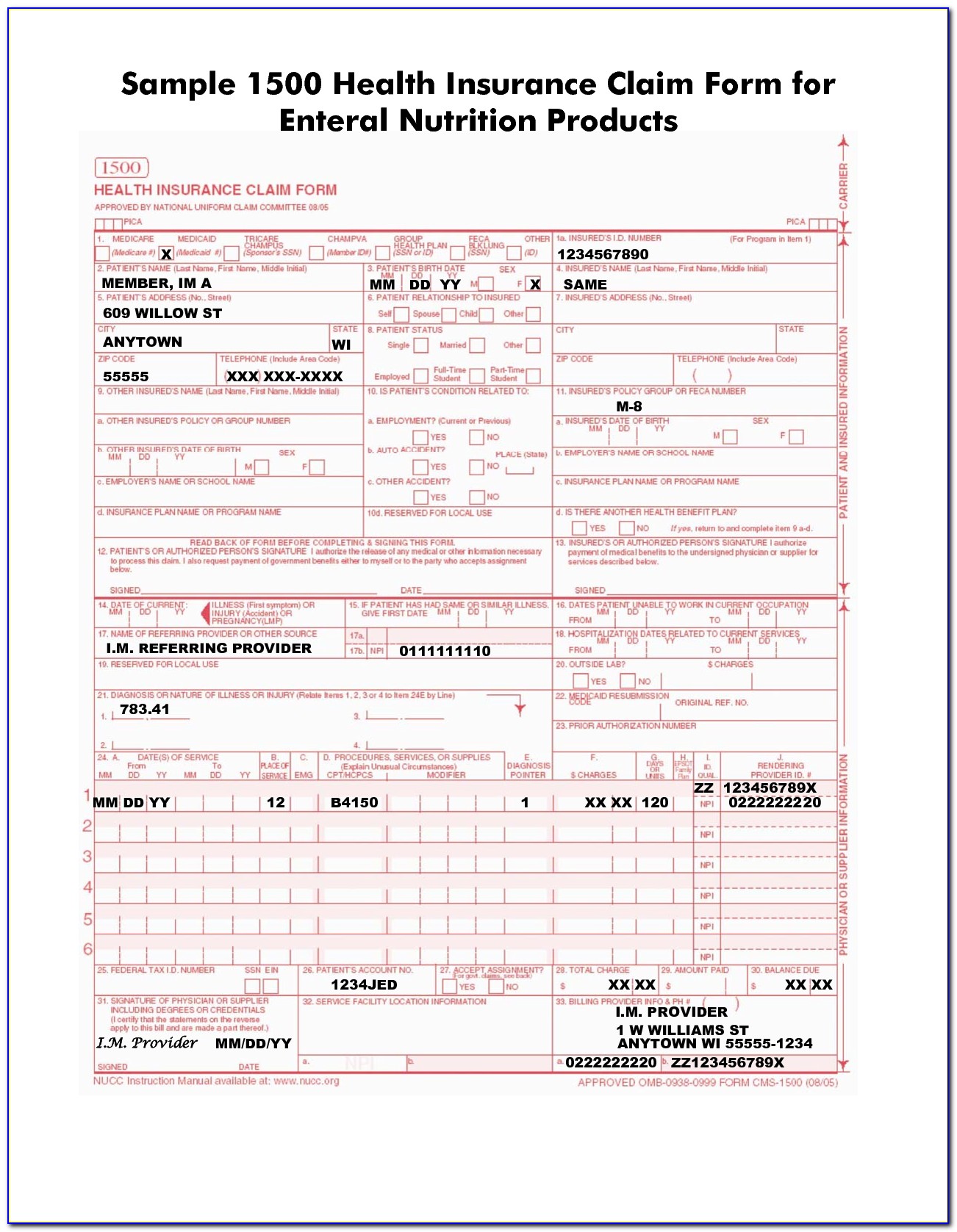
Hcfa 1500 Form Printable - It is the basic form prescribed by hcfa for the medicare program for claims from physicians and suppliers, except for ambulance services. Let's take a look at both. You can decide how often to. Item 6 patient’s relationship to insured if medicare is primary, leave blank. Web no part b medicare benefits may be paid unless this form is received as required by existing law and regulations (42 cfr 424.32). Number (for program in item 1) 4. It is also used by private insurers and managed care plans; Tips for printing your claim form. If the user would like to complete the form online, simply download, click inside the box to begin and begin typing your information. Decide on what kind of signature to create.
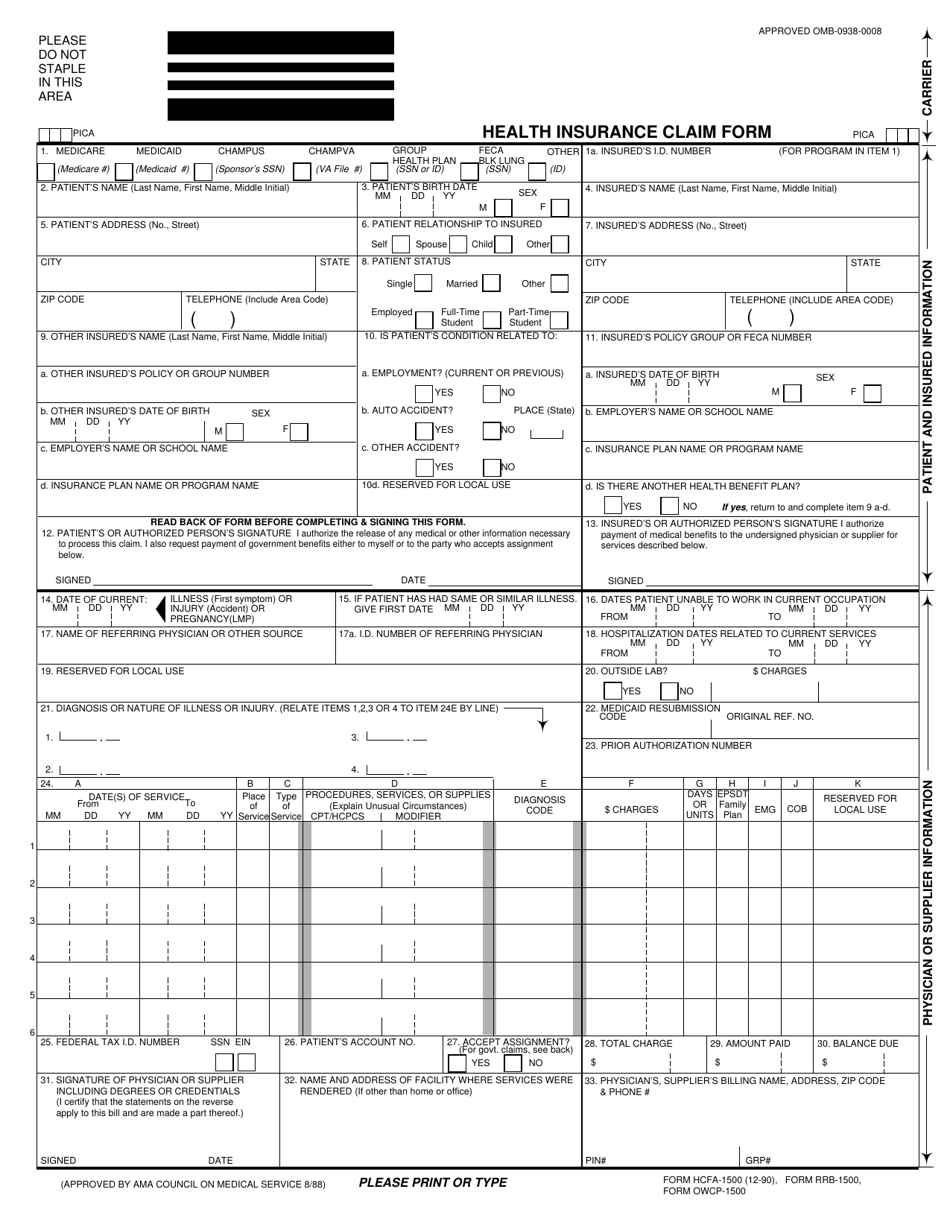
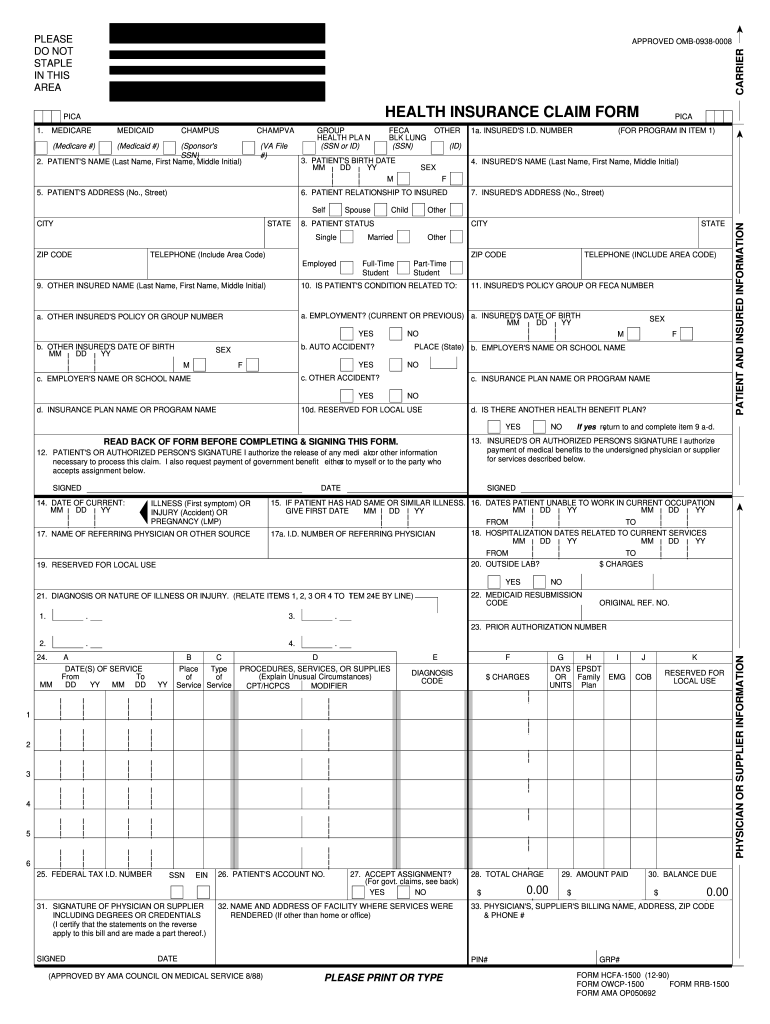
After that, your cfa claim form is ready. Please mail them to the name and address listed here. We are authorized by hcfa, champus. A typed, drawn or uploaded signature. Web download the fillable hcfa 1500 claim form that is both a fillable and/or printable medical claim form that will provide insurance, illness and injury information for medical services claims. Insured’s name (last name, first name, middle initial) 7. Managed care the official standard form used by physicians and other providers when submitting bills/claims for reimbursement to medicare or medicaid for health services; Item 6 patient’s relationship to insured if medicare is primary, leave blank. Number (for program in item 1) 4. Because this form is used by various government and private health programs, see separate instructions issued by applicable programs.
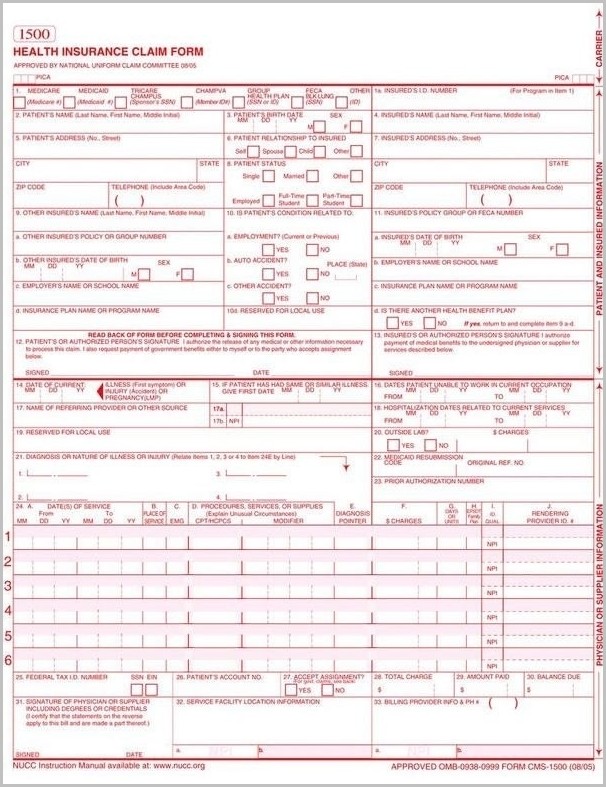
Be sure to select the new template as the default template before exiting the screen. Web download the fillable hcfa 1500 claim form that is both a fillable and/or printable medical claim form that will provide insurance, illness and injury information for medical services claims. Printing your cms 1500 form. Download hcfa 1500 today for free! It is also used by private insurers and managed care plans; Web february 09, 2023 17:28. Web the 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. You can decide how often to. It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers,. Insured’s name (last name, first name, middle initial) 7.
Hcfa 1500 Form Aflac Form Resume Examples NEpDLQE5xR
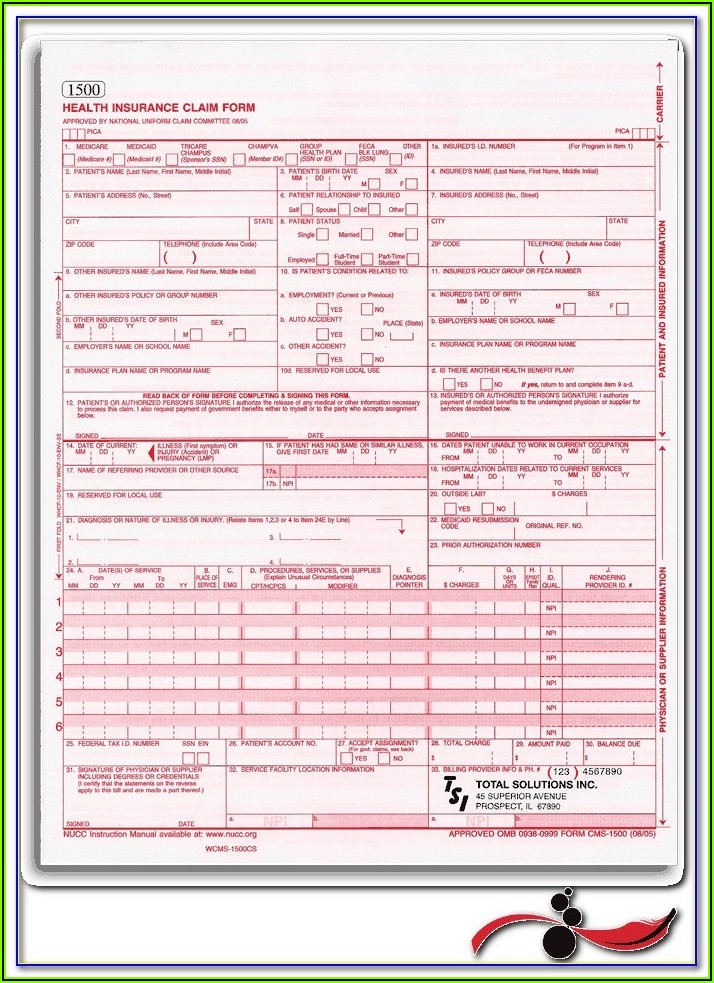
Web trying to find hcfa 1500? Web hcfa 1500 form printable. Managed care the official standard form used by physicians and other providers when submitting bills/claims for reimbursement to medicare or medicaid for health services; Web download the fillable hcfa 1500 claim form that is both a fillable and/or printable medical claim form that will provide insurance, illness and injury.
Hcfa 1500 Claim Form Printable Form Resume Examples P32ERx49J8
Be sure to select the new template as the default template before exiting the screen. Here, you can get this form and modify or fill it out with our pdf tool online. Download free cms 1500 claim form fillable template. In this guide, we'll cover: Decide on what kind of signature to create.

Hcfa 1500 Forms Free Download Form Resume Examples Or85MMO8Wz
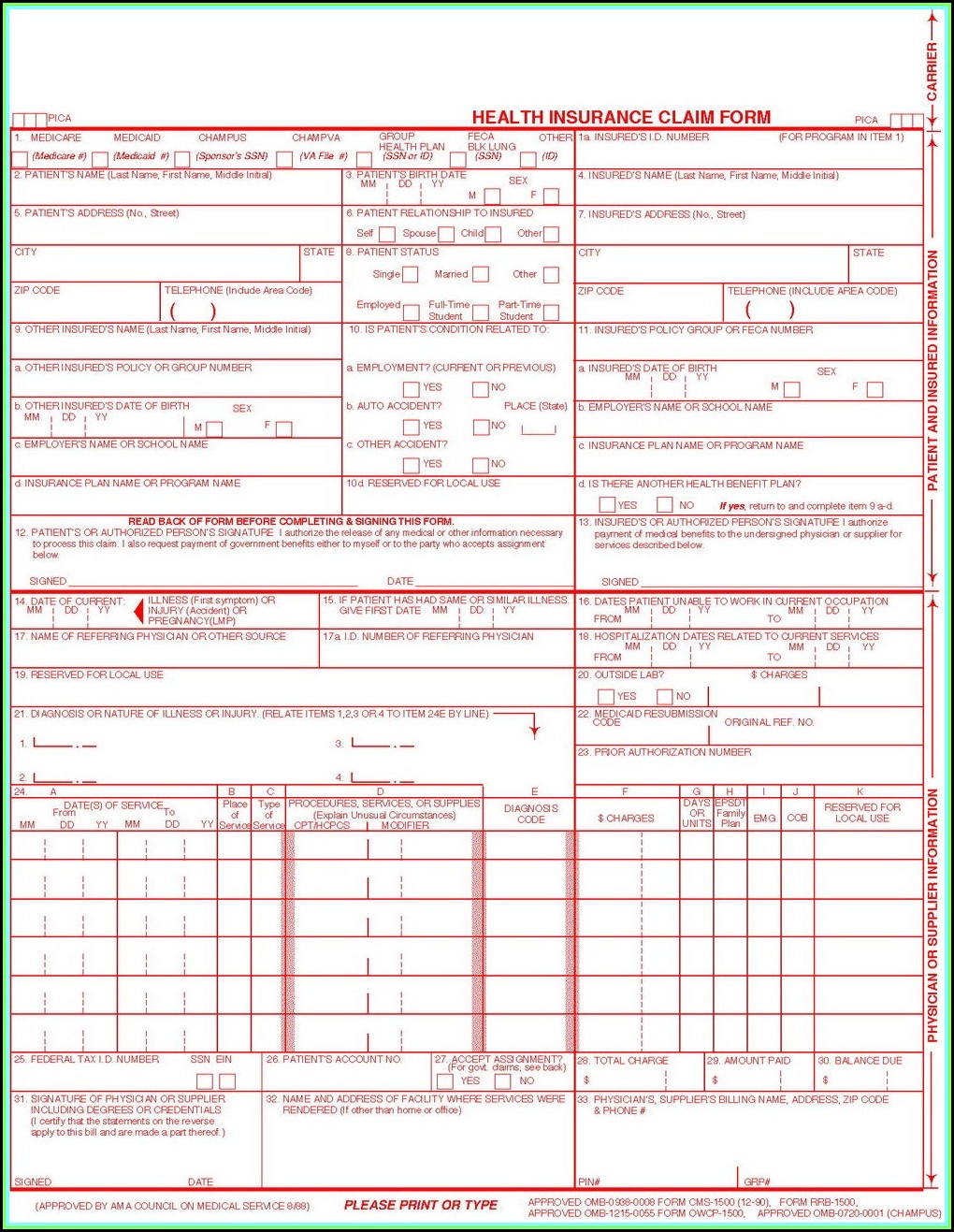
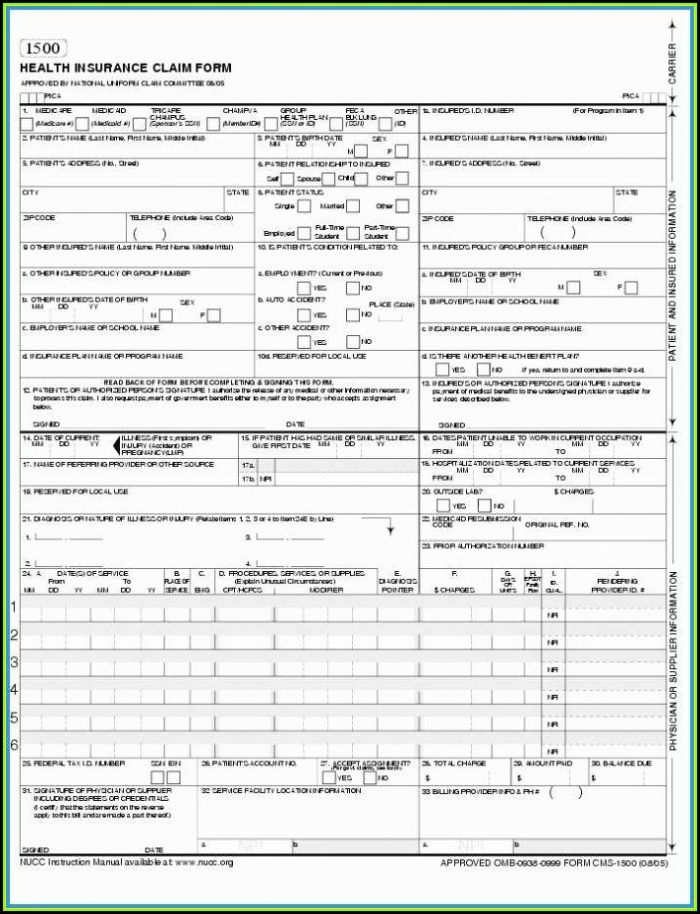
Insured’s address (no., street) city state zip code telephone (include area code) 11. Web a hcfa 1500 form is used by the health care financing administration. Web download the fillable hcfa 1500 claim form that is both a fillable and/or printable medical claim form that will provide insurance, illness and injury information for medical services claims. We are authorized by.
Example Of Hcfa 1500 Claim Form Form Resume Examples kLYrAOw96a
Download hcfa 1500 today for free! It is used to submit a bill or charge for health insurance coverage. Web the 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Get everything done in minutes. Item 7 insurance primary to medicare, insured’s address and telephone number complete this item only when items 4,.
Form Hcfa 1500 Form Resume Examples 4x2v1DQV5l
The current version of the original manual from the national uniform claim comettee of how to complete the cms1500 claim form. If the user would like to complete the form online, simply download, click inside the box to begin and begin typing your information. Download hcfa 1500 today for free! In this guide, we'll cover: Web the 1500 health insurance.
Hcfa 1500 Claim Form Aflac Form Resume Examples EvkBj86k2d
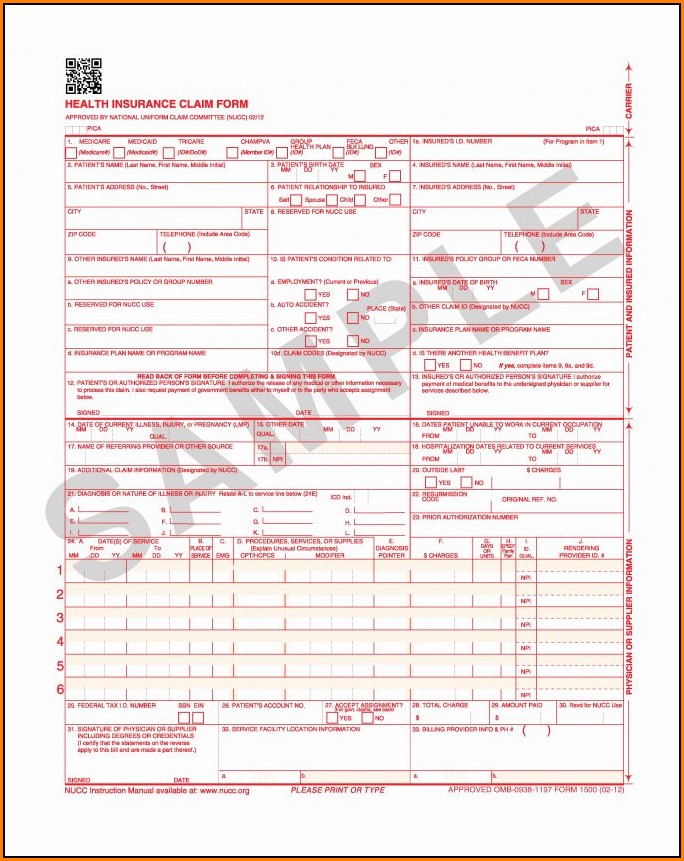
Web february 09, 2023 17:28. Sign up to get the latest information about your choice of cms topics. Read the instructions and tips below first. Hcfa 1500 contains pt demographics, diagnostic codes, cpt/hcpcs codes, diagnosis codes, units. Web hcfa 1500 form printable.
Hcfa 1500 Form Sample Form Resume Examples
Sign up to get the latest information about your choice of cms topics. You can decide how often to. Item 7 insurance primary to medicare, insured’s address and telephone number complete this item only when items 4, 6, and 11 are. Read the instructions and tips below first. Insured’s name (last name, first name, middle initial) 7.
Medicare Billing Form Hcfa 1500cms 1500 Form Resume Examples
A typed, drawn or uploaded signature. You can decide how often to. Web a hcfa 1500 form is used by the health care financing administration. When you receive your explanation of medicare benefits papers, attach copies to your hcfa 1500 claim forms. The advanced tools of the editor will direct you through the editable pdf template.
Form HCFA1500 Download Printable PDF or Fill Online Health Insurance
Tips for printing your claim form. Hcfa 1500 contains pt demographics, diagnostic codes, cpt/hcpcs codes, diagnosis codes, units. Web how to complete the form hcfa1500 on the internet: Web no part b medicare benefits may be paid unless this form is received as required by existing law and regulations (42 cfr 424.32). It is also used by private insurers and.
Hcfa Form Fill Out and Sign Printable PDF Template signNow
When you receive your explanation of medicare benefits papers, attach copies to your hcfa 1500 claim forms. Item 7 insurance primary to medicare, insured’s address and telephone number complete this item only when items 4, 6, and 11 are. Creating a cms 1500 form. Sign up to get the latest information about your choice of cms topics. Check the appropriate.
Hcfa 1500 Contains Pt Demographics, Diagnostic Codes, Cpt/Hcpcs Codes, Diagnosis Codes, Units.
After that, your cfa claim form is ready. You can decide how often to. Any one who misrepresents or falsifies essential information to receive payment from federal funds requested by this form may upon conviction be subject to fine and imprisonment under applicable federal laws. Select the document you want to sign and click upload.
If The User Would Like To Complete The Form Online, Simply Download, Click Inside The Box To Begin And Begin Typing Your Information.
Web download the fillable hcfa 1500 claim form that is both a fillable and/or printable medical claim form that will provide insurance, illness and injury information for medical services claims. Web hcfa 1500 form printable. Number (for program in item 1) 4. Download free cms 1500 claim form fillable template.
Printing Your Cms 1500 Form.
Please mail them to the name and address listed here. Item 7 insurance primary to medicare, insured’s address and telephone number complete this item only when items 4, 6, and 11 are. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Web no part b medicare benefits may be paid unless this form is received as required by existing law and regulations (42 cfr 424.32).
Insured’s Name (Last Name, First Name, Middle Initial) 7.
Insured’s address (no., street) city state zip code telephone (include area code) 11. Web the 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Sign up to get the latest information about your choice of cms topics. The current version of the original manual from the national uniform claim comettee of how to complete the cms1500 claim form.