Health Alliance Appeal Form
Health Alliance Appeal Form - Web appeals, grievances, & hearings. Web this form can be used to ask alliance to reconsider a decision to deny a service request. Web request form medical records must accompany all requests to be completed for all requests. Umpqua health alliance (uha) cares about you and your health. Web for information on submitting claims, visit our updated where to submit claims webpage. Web health alliance credentialing application (for contracted midlevel providers) caqh provider addition form (for il contracted mds and dos only) ancillary facility checklist. Web the provider request for reconsideration form is posted on the alliance web site and serves as a cover page to the provider appeal. Provider network management section 3: Please include any supporting documents, notes, statements, and medical. Cotiviti and change healthcare/tc3 claims denial appeal form;
Web member appeal form complete this form if you are appealing the outcome of a processed medical need. Here are forms you'll need: Web request form medical records must accompany all requests to be completed for all requests. Incomplete or illegible information will. Web a written request for a reconsideration of the decision must be submitted to health alliance within 60 days from the date of denial notice from health alliance. Complete the form below with your alliance information. Please include any supporting documents, notes, statements, and medical. Web health alliance credentialing application (for contracted midlevel providers) caqh provider addition form (for il contracted mds and dos only) ancillary facility checklist. Cotiviti and change healthcare/tc3 claims denial appeal form; The questions and answers below will provide additional information and instruction.
Web appeals, grievances, & hearings. Web our process for accepting and responding to appeals. Web community care network contact centerproviders and va staff only. Web the provider request for reconsideration form is posted on the alliance web site and serves as a cover page to the provider appeal. Web request form medical records must accompany all requests to be completed for all requests. Web this form can be used to ask alliance to reconsider a decision to deny a service request. Provider network management section 3: Web a written request for a reconsideration of the decision must be submitted to health alliance within 60 days from the date of denial notice from health alliance. The questions and answers below will provide additional information and instruction. To 8 p.m., monday through friday;

Health Alliance Medicare Prior Authorization Form Doctor Heck
To 8 p.m., monday through friday; Alliance will acknowledge receipt of. Web member appeal form complete this form if you are appealing the outcome of a processed medical need. The questions and answers below will provide additional information and instruction. If we deny your request for a coverage decision or payment, you have the right to request an appeal.

Cigna Appeal Form Fill Online, Printable, Fillable, Blank pdfFiller
Web appeals, grievances, & hearings. Drug deaths nationwide hit a record. Of health and human services (hhs) grant. Web health alliance credentialing application (for contracted midlevel providers) caqh provider addition form (for il contracted mds and dos only) ancillary facility checklist. Web we want it to be easy for you to work with hap.

Health Alliance Appeal Form Doctor Heck
Web to submit a formal appeal, you must complete the provider appeal form located at provider.healthalliance.org. The questions and answers below will provide additional information and instruction. Web appeals, grievances, & hearings. Web member appeal form complete this form if you are appealing the outcome of a processed medical need. Web the provider request for reconsideration form is posted on.
Cal Osha Appeal's Form C Om Fill Out and Sign Printable PDF Template
Web community care network contact centerproviders and va staff only. Web this handout was developed in part under a grant from the health resources and services administration (hrsa), u.s. Is facing intensifying urgency to stop the worsening fentanyl epidemic. Web member appeal form complete this form if you are appealing the outcome of a processed medical need. Web for information.
Wellcare Appeal Form Fill Online, Printable, Fillable, Blank pdfFiller
Complete the form below with your alliance information. Web here you’ll find forms relating to your medicare plan. Web we want it to be easy for you to work with hap. Web request form medical records must accompany all requests to be completed for all requests. Umpqua health alliance (uha) cares about you and your health.
Home Health Referral Form Template Fill Out and Sign Printable PDF
Provider network management section 3: Is facing intensifying urgency to stop the worsening fentanyl epidemic. Please choose the type of. Web for dates of service august 1, 2021 and after, the appeals process will now have one level of formal appeal after first asking for an informal inquiry on a denied. Please include any supporting documents, notes, statements, and medical.
Indiana Medicaid Appeal Form Fill Online, Printable, Fillable, Blank
Web appeals, grievances, & hearings. Web the hearing was particularly timely, because the u.s. Web community care network contact centerproviders and va staff only. Web for dates of service august 1, 2021 and after, the appeals process will now have one level of formal appeal after first asking for an informal inquiry on a denied. Web health alliance credentialing application.
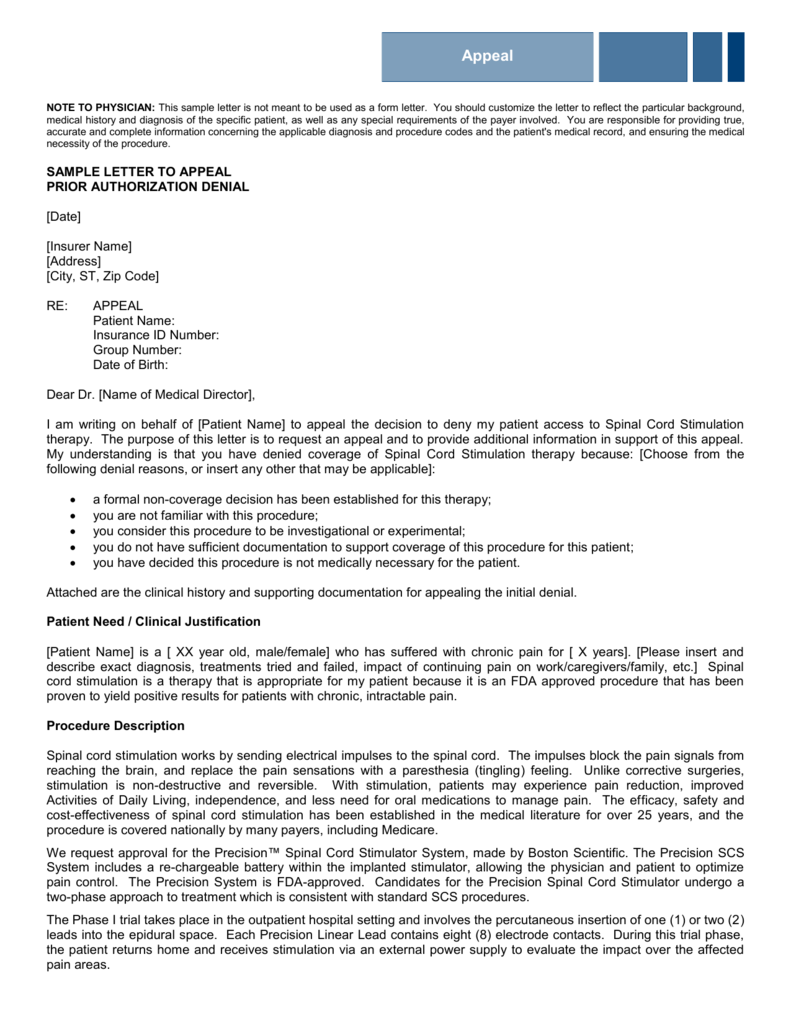
Sample Appeal Letter For Medical Claim Denial designerwrapper
Web this form can be used to ask alliance to reconsider a decision to deny a service request. Alliance will acknowledge receipt of. Web for dates of service august 1, 2021 and after, the appeals process will now have one level of formal appeal after first asking for an informal inquiry on a denied. Web to file or check the.

Health Insurance Marketplace Appeal Request Form 0 Printable Blank
Web we want it to be easy for you to work with hap. Provider network management section 3: Web for dates of service august 1, 2021 and after, the appeals process will now have one level of formal appeal after first asking for an informal inquiry on a denied. Web request form medical records must accompany all requests to be.
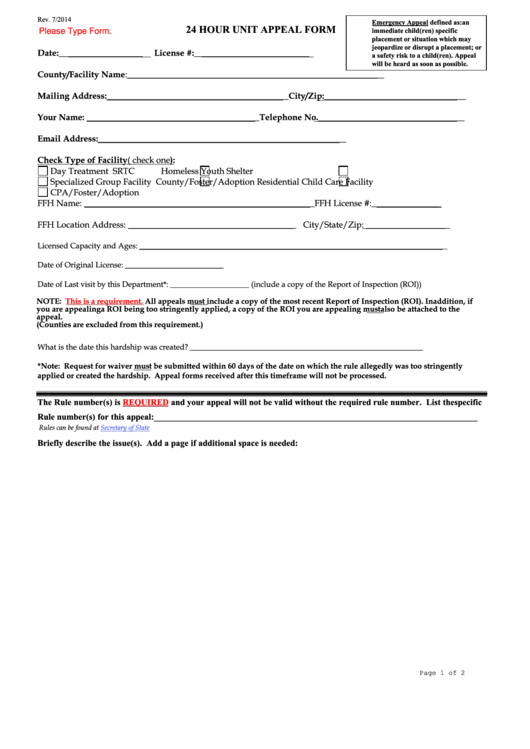
Fillable 24 Hour Unit Appeal Form Colorado Department Of Human
Web community care network contact centerproviders and va staff only. If we deny your request for a coverage decision or payment, you have the right to request an appeal. Once the appeal form has been completed,. Web request form medical records must accompany all requests to be completed for all requests. Please choose the type of.
Here Are Forms You'll Need:
Alliance will acknowledge receipt of. In your local time zone. Uha and our providers will not stop you from filing a complaint, appeal or hearing. Web community care network contact centerproviders and va staff only.
Web To Submit A Formal Appeal, You Must Complete The Provider Appeal Form Located At Provider.healthalliance.org.
Please include any supporting documents, notes, statements, and medical. Web health alliance credentialing application (for contracted midlevel providers) caqh provider addition form (for il contracted mds and dos only) ancillary facility checklist. Web for dates of service august 1, 2021 and after, the appeals process will now have one level of formal appeal after first asking for an informal inquiry on a denied. Web this form can be used to ask alliance to reconsider a decision to deny a service request.
Web Request Form Medical Records Must Accompany All Requests To Be Completed For All Requests.
Web the provider request for reconsideration form is posted on the alliance web site and serves as a cover page to the provider appeal. Complete the form below with your alliance information. Once the appeal form has been completed,. Drug deaths nationwide hit a record.
Web To File Or Check The Status Of A Grievance Or An Appeal‚ Contact Us At:
Web appeals, grievances, & hearings. Cotiviti and change healthcare/tc3 claims denial appeal form; Provider network management section 3: Umpqua health alliance (uha) cares about you and your health.