Highmark Bcbs Prior Authorization Form
Highmark Bcbs Prior Authorization Form - The list includes services such as: Some authorization requirements vary by member contract. Web highmark requires authorization of certain services, procedures, and/or durable medical equipment, prosthetics, orthotics, & supplies ( dmepos) prior to performing the procedure or service. Web to search for a specific procedure code on the list of procedures/dme requiring authorization, press control key + f key, enter the procedure code and press enter. Note:the prescribing physician (pcp or specialist) should, in most cases, complete the form. Designation of authorized representative form. Web independent blue cross blue shield plans. Potentially experimental, investigational, or cosmetic services select. Inpatient and outpatient authorization request form. Web highmark blue cross blue shield of western new york (highmark bcbswny) requires authorization of certain services, procedures, and/or dmepos prior to performing the procedure or service.
Web highmark blue cross blue shield of western new york (highmark bcbswny) requires authorization of certain services, procedures, and/or dmepos prior to performing the procedure or service. Web for a complete list of services requiring authorization, please access the authorization requirements page on the highmark provider resource center under claims, payment & reimbursement > procedure/service requiring prior authorization or by the following link: Some authorization requirements vary by member contract. Inpatient and outpatient authorization request form. A physician must fill in the form with the patient’s member information as well as all medical details related to the requested prescription. Or contact your provider account liaison. Some authorization requirements vary by member contract. Web independent blue cross blue shield plans. Potentially experimental, investigational, or cosmetic services select. Web to search for a specific procedure code on the list of procedures/dme requiring authorization, press control key + f key, enter the procedure code and press enter.
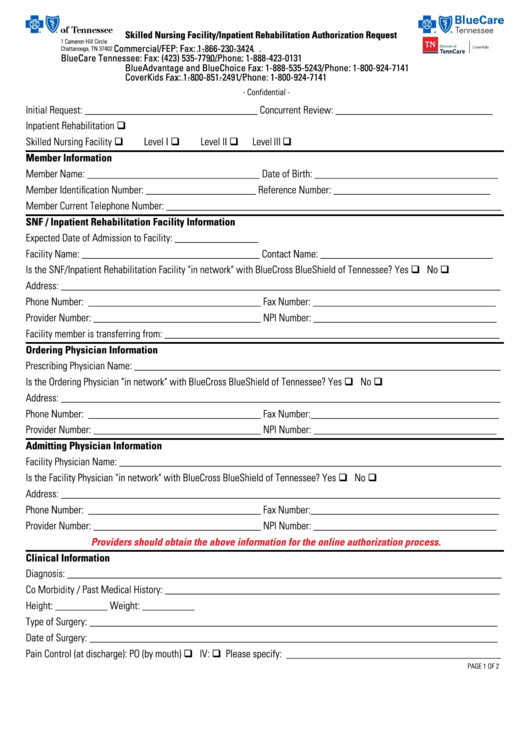
Use this form for all physical, occupational, speech, and feeding therapies, pulmonary and cardiac rehabilitation, and chiropractic care. Web for a complete list of services requiring authorization, please access the authorization requirements page on the highmark provider resource center under claims, payment & reimbursement > procedure/service requiring prior authorization or by the following link: The list includes services such as: Web provider manual and resources forms and reference material forms and reference material forms and reports picture_as_pdf abortion consent form picture_as_pdf advance directive form picture_as_pdf applied behavioral analysis (aba) prior authorization request form attendant care monthly missed visits/hours/shifts report Complete all information on the form. Web independent blue cross blue shield plans. The authorization is typically obtained by the ordering provider. Some authorization requirements vary by member contract. Web we can help. Note:the prescribing physician (pcp or specialist) should, in most cases, complete the form.
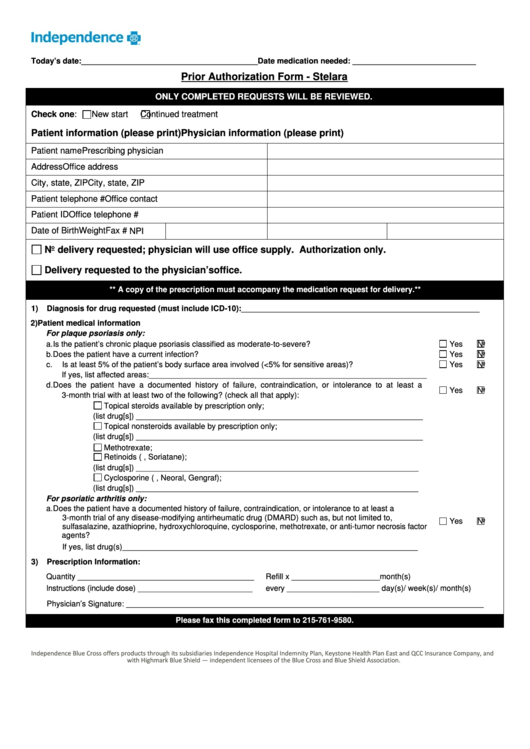
Independence Prior Authorization Form Stelara printable pdf download
Web highmark requires authorization of certain services, procedures, and/or durable medical equipment, prosthetics, orthotics, & supplies ( dmepos) prior to performing the procedure or service. Designation of authorized representative form. Note:the prescribing physician (pcp or specialist) should, in most cases, complete the form. Use this form for all physical, occupational, speech, and feeding therapies, pulmonary and cardiac rehabilitation, and chiropractic.
Top 28 Blue Cross Blue Shield Prior Authorization Form Templates free
Web we can help. Web highmark blue cross blue shield of western new york (highmark bcbswny) requires authorization of certain services, procedures, and/or dmepos prior to performing the procedure or service. Complete all information on the form. The authorization is typically obtained by the ordering provider. Web independent blue cross blue shield plans.
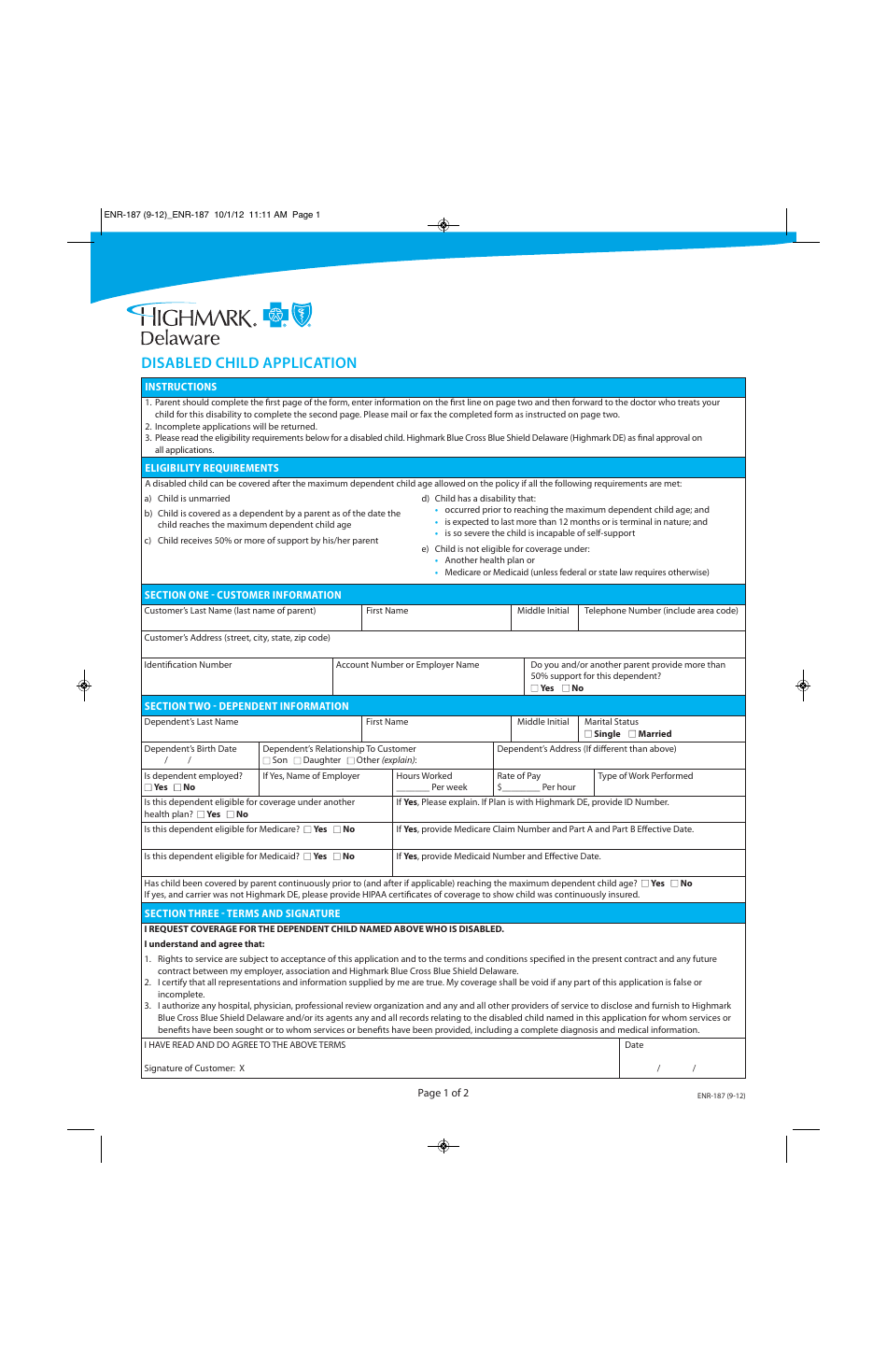
Form ENR187 Download Printable PDF or Fill Online Disabled Child
Web we can help. Potentially experimental, investigational, or cosmetic services select. Designation of authorized representative form. Use this form for all physical, occupational, speech, and feeding therapies, pulmonary and cardiac rehabilitation, and chiropractic care. Submit a separate form for each medication.

About Privacy Policy Copyright TOS Contact Sitemap
Review the prior authorizations section of the provider manual. Designation of authorized representative form. Web highmark requires authorization of certain services, procedures, and/or durable medical equipment, prosthetics, orthotics, & supplies ( dmepos) prior to performing the procedure or service. Or contact your provider account liaison. Web we can help.
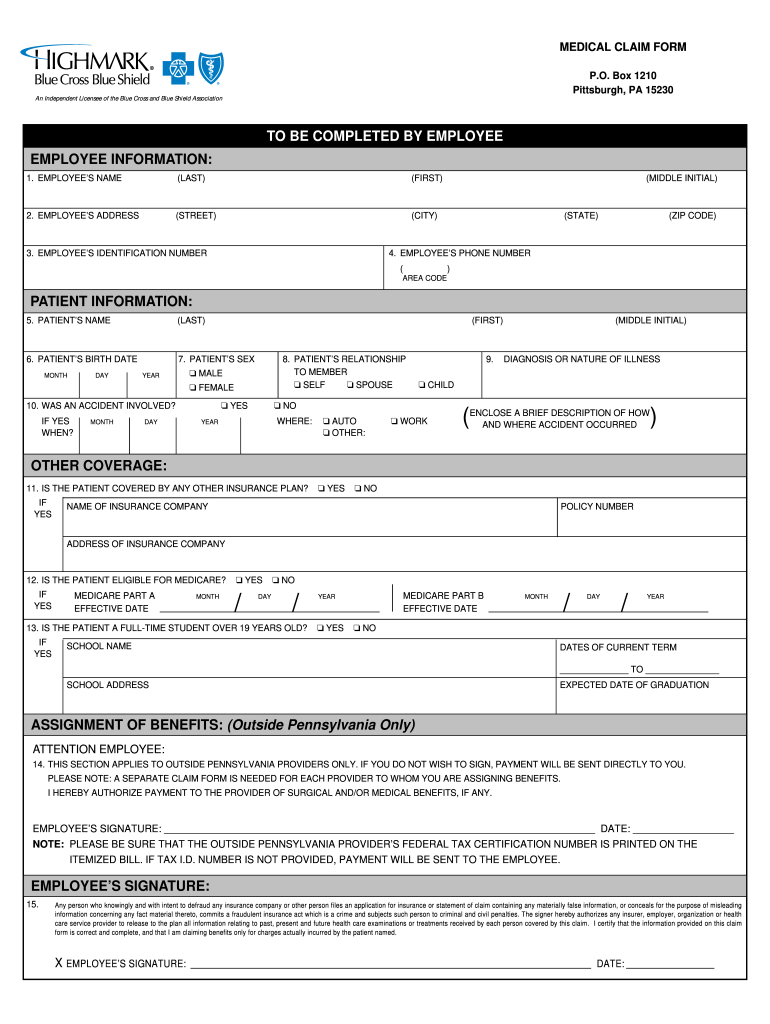
Highmark BCBS CLM038 2000 Fill and Sign Printable Template Online
Please provide the physician address as it is required for physician notification. Complete all information on the form. Review the prior authorizations section of the provider manual. Web provider manual and resources forms and reference material forms and reference material forms and reports picture_as_pdf abortion consent form picture_as_pdf advance directive form picture_as_pdf applied behavioral analysis (aba) prior authorization request form.
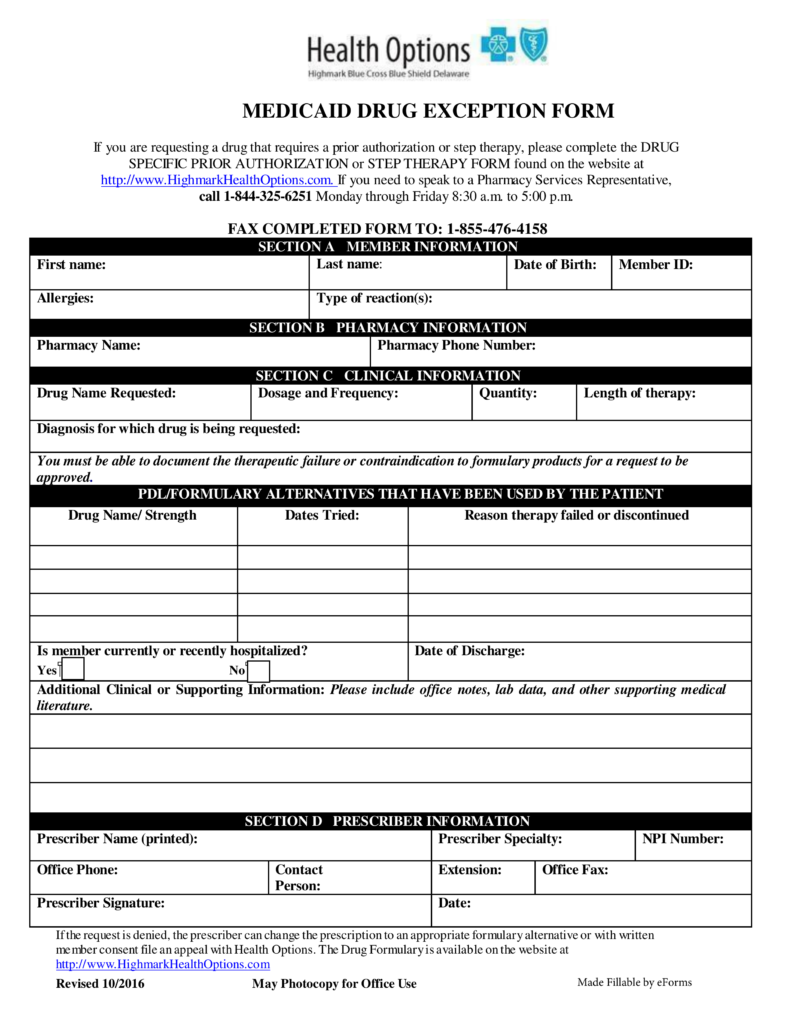
Free Delaware Medicaid Prior (Rx) Authorization Form PDF eForms
Some authorization requirements vary by member contract. Web independent blue cross blue shield plans. Please provide the physician address as it is required for physician notification. Complete all information on the form. Web provider manual and resources forms and reference material forms and reference material forms and reports picture_as_pdf abortion consent form picture_as_pdf advance directive form picture_as_pdf applied behavioral analysis.

Highmark blue shield prescription forms
Some authorization requirements vary by member contract. Complete all information on the form. Note:the prescribing physician (pcp or specialist) should, in most cases, complete the form. Some authorization requirements vary by member contract. Potentially experimental, investigational, or cosmetic services select.

Gallery of Highmark Bcbs Medication Prior Authorization form Lovely
Web a highmark prior authorization form is a document used to determine whether a patient’s prescription cost will be covered by their highmark health insurance plan. Inpatient and outpatient authorization request form. Web to search for a specific procedure code on the list of procedures/dme requiring authorization, press control key + f key, enter the procedure code and press enter..
Bcbs Prior Authorization Form For Radiology Form Resume Examples
A physician must fill in the form with the patient’s member information as well as all medical details related to the requested prescription. The authorization is typically obtained by the ordering provider. Potentially experimental, investigational, or cosmetic services select. The list includes services such as: Web provider manual and resources forms and reference material forms and reference material forms and.

Gallery of Highmark Bcbs Medication Prior Authorization form Lovely
Potentially experimental, investigational, or cosmetic services select. Submit a separate form for each medication. Complete all information on the form. Web a highmark prior authorization form is a document used to determine whether a patient’s prescription cost will be covered by their highmark health insurance plan. The list includes services such as:
Review The Prior Authorizations Section Of The Provider Manual.
Web a highmark prior authorization form is a document used to determine whether a patient’s prescription cost will be covered by their highmark health insurance plan. Web for a complete list of services requiring authorization, please access the authorization requirements page on the highmark provider resource center under claims, payment & reimbursement > procedure/service requiring prior authorization or by the following link: Designation of authorized representative form. The authorization is typically obtained by the ordering provider.
A Physician Must Fill In The Form With The Patient’s Member Information As Well As All Medical Details Related To The Requested Prescription.
Please provide the physician address as it is required for physician notification. Web independent blue cross blue shield plans. Web highmark blue cross blue shield of western new york (highmark bcbswny) requires authorization of certain services, procedures, and/or dmepos prior to performing the procedure or service. Submit a separate form for each medication.
Some Authorization Requirements Vary By Member Contract.
Some authorization requirements vary by member contract. Inpatient and outpatient authorization request form. Web provider manual and resources forms and reference material forms and reference material forms and reports picture_as_pdf abortion consent form picture_as_pdf advance directive form picture_as_pdf applied behavioral analysis (aba) prior authorization request form attendant care monthly missed visits/hours/shifts report Note:the prescribing physician (pcp or specialist) should, in most cases, complete the form.
Use This Form For All Physical, Occupational, Speech, And Feeding Therapies, Pulmonary And Cardiac Rehabilitation, And Chiropractic Care.
Web to search for a specific procedure code on the list of procedures/dme requiring authorization, press control key + f key, enter the procedure code and press enter. Potentially experimental, investigational, or cosmetic services select. Or contact your provider account liaison. The authorization is typically obtained by the ordering provider.