Hipaa Release Form Maryland
Hipaa Release Form Maryland - Don’t delay, try for free today! Unless the recipient is covered by maryland law which prohibits redisclosure or other. Web iac compliance privacy and hipaa institutional review board (irb) mdh records management office strategic data initiative (sdi) privacy and hipaa mdh privacy matters are handled through the privacy officer within iac's compliance division. Web authorization form for release of records and information page 3. Keep it simple when filling out your maryland hipaa medical authorization release form pdf and use pdfsimpli. Keep a copy of this completed form for your records. Web the hipaa law was enacted to ensure your healthcare information remains private. Web authorization for the release of medical information. [check as appropriate] from or to from or university of maryland university health center For additional information and resources, visit the mhcc cybersecurity webpage.
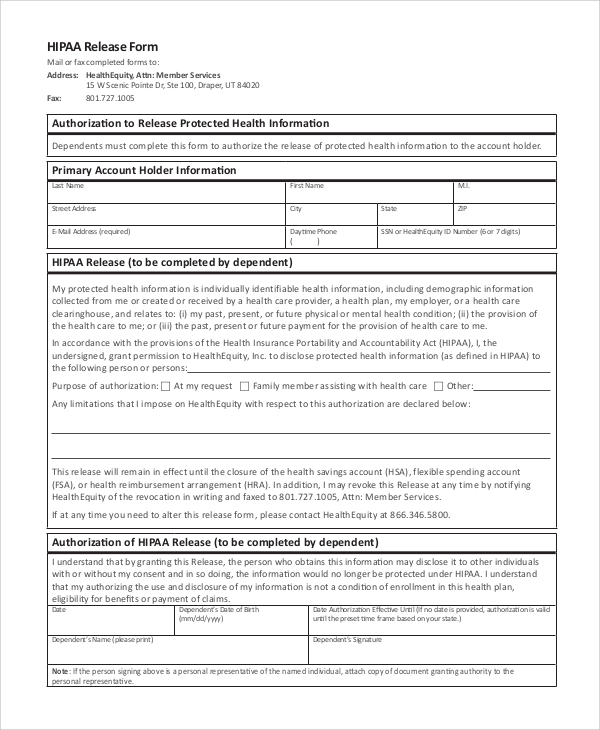
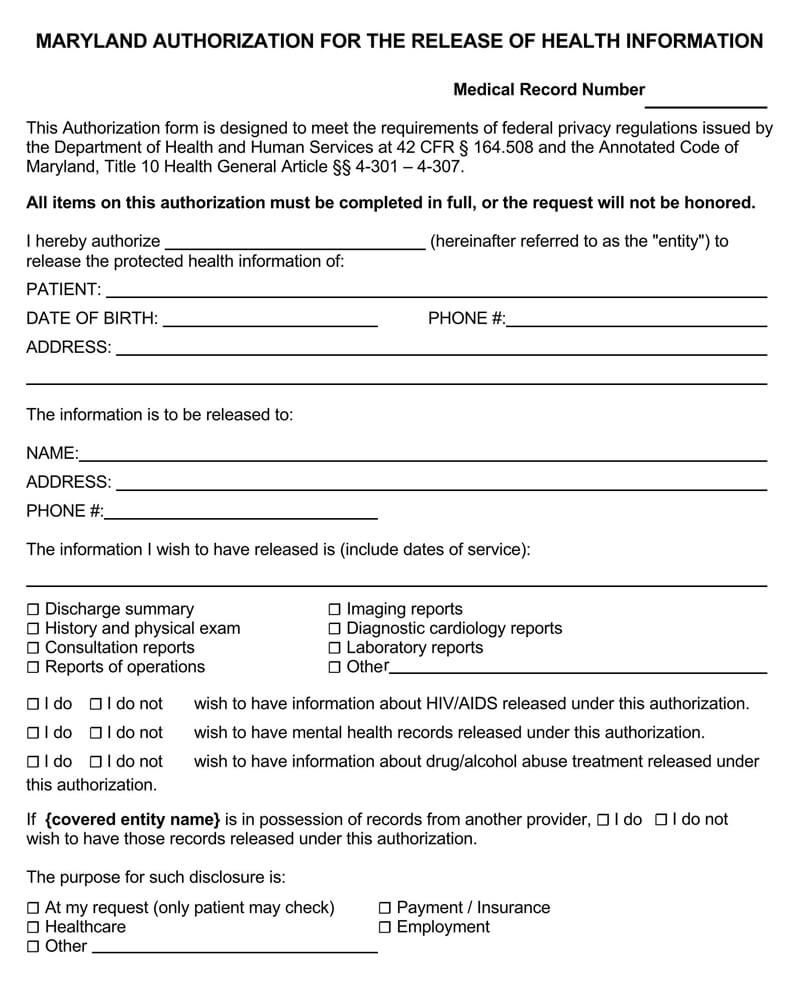
You can email us your form at ummsrelease@umm.edu. Web this document compares the similarities and differences in regulations addressing privacy of health care information between the maryland confidentiality of medical records act (mcrma) and hipaa. All items on this authorization must be completed in full, or the request will not be honored. The release also allows the added option for healthcare providers to share information. Employee benefits division, hipaa privacy officer, room 510, 301 w. Web fill out the maryland hipaa medical authorization release form pdf form for free! Cy21 pa group hipaa authorization form author: Submit request (authorization release form) please mail or fax your authorization release form. Web hipaa regulations require that patient documents must be kept a minimum of six (6) years. Authorization for release of information phone:
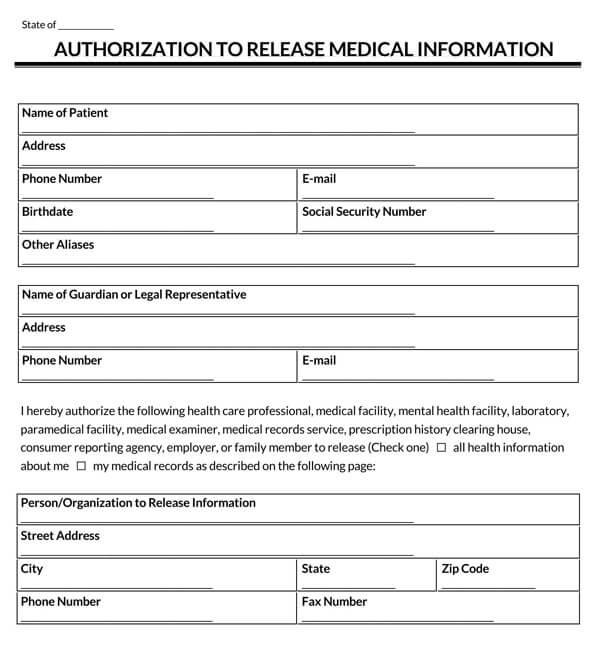
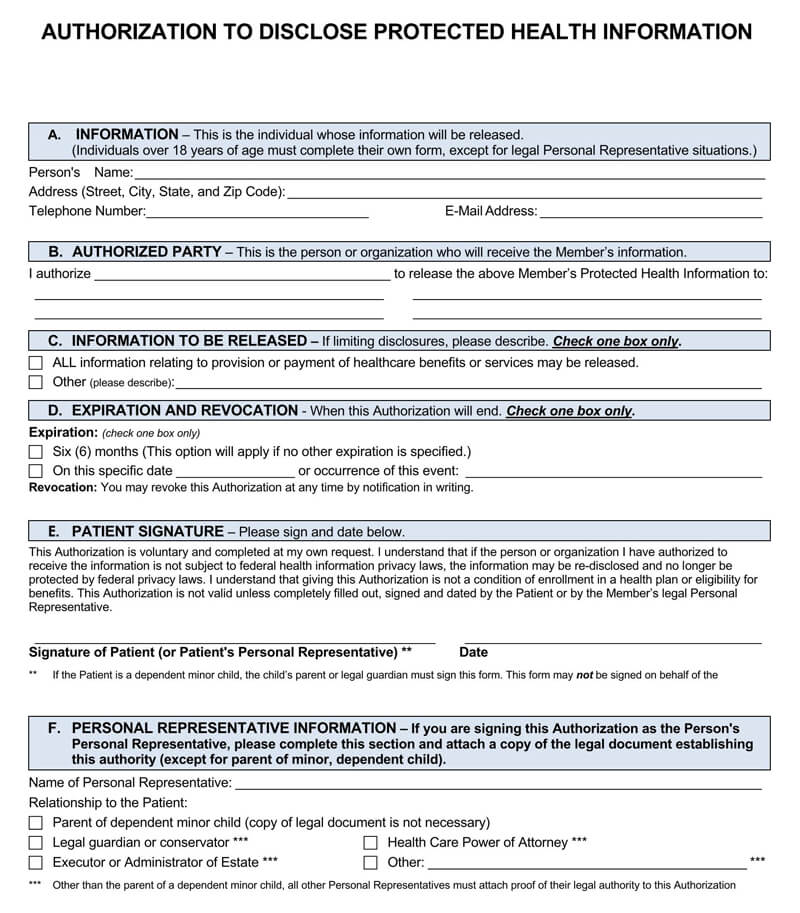
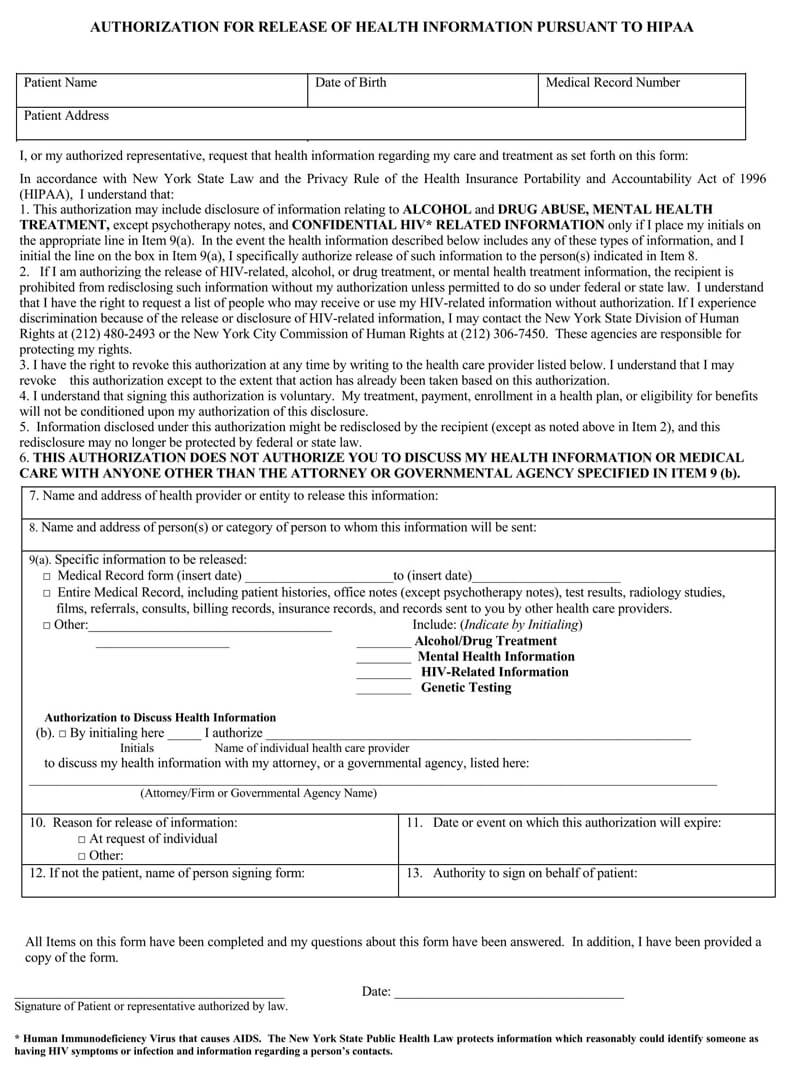
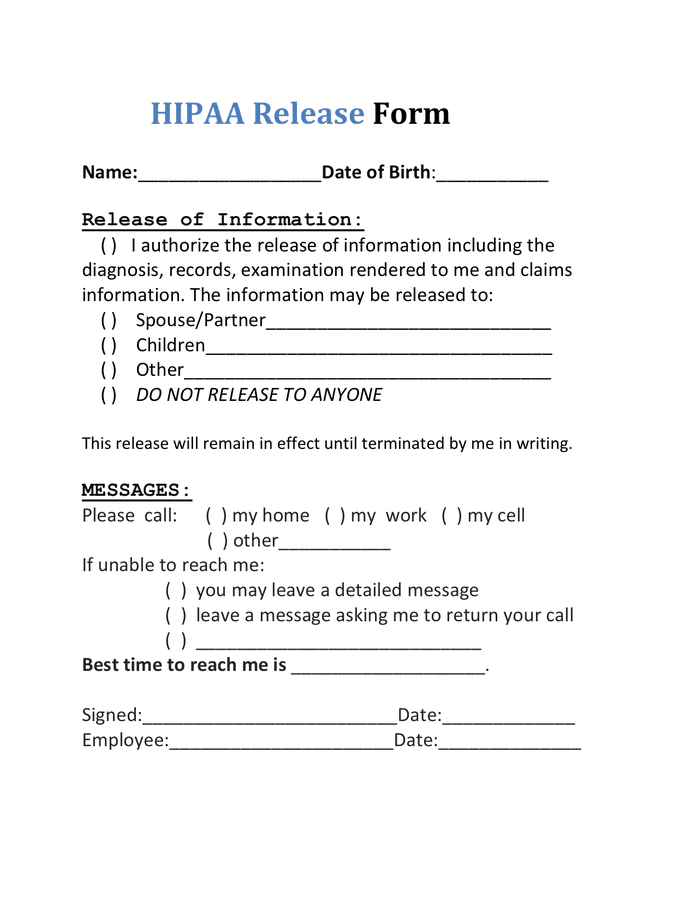
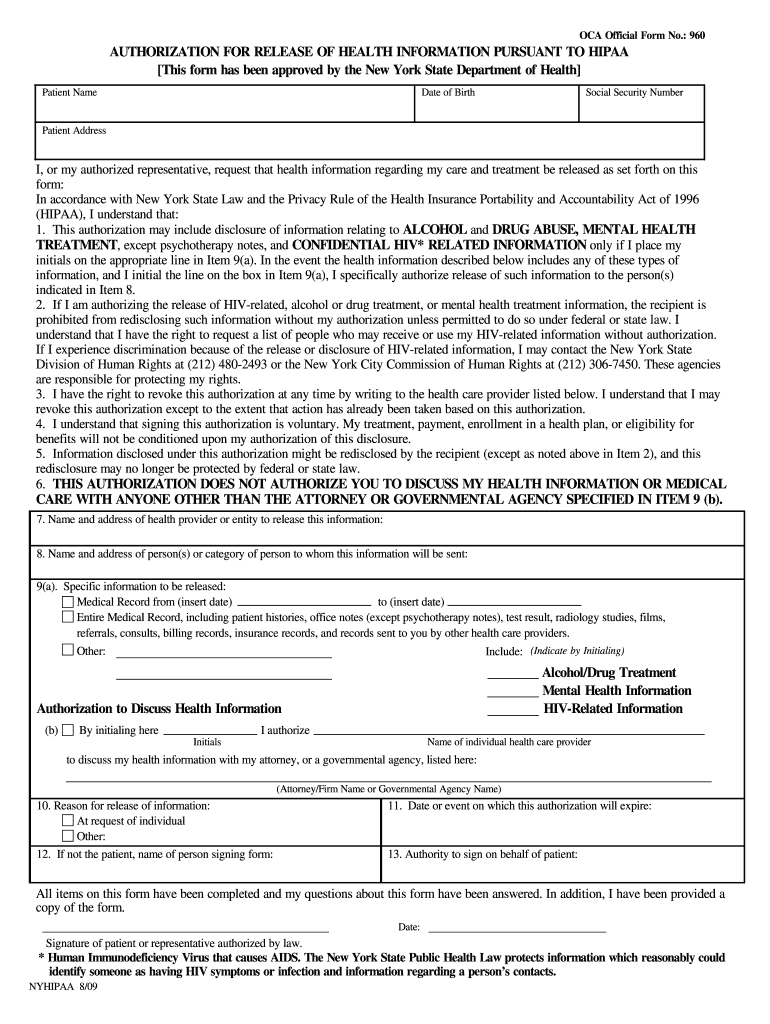
Web the hipaa law was enacted to ensure your healthcare information remains private. You must continue on the next page authorization form for release of records and information page 3 Web authorization for the release of medical information. Web the medical record information release (hipaa) form allows a patient to give authorization to a 3rd party and access their health records. Web to revoke the authorization, i understand i must contact the following in writing: All items on this form have been completed and my questions about this form have been answered. At request of individual other: Web 10.reason for release of information: All items on this authorization must be completed in full, or the request will not be honored. Web patient authorization to release protected health information (phi) patient name:
Free HIPAA Medical Records Release Forms (U.S) PDF Word
Please include your name in the subject line. If not the patient, name of person signing form: Hereby authorize the disclosure and use of my health information: The release also allows the added option for healthcare providers to share information. Employee benefits division, hipaa privacy officer, room 510, 301 w.
Free Medical Records Release Authorization Forms (HIPAA)
Unless the recipient is covered by maryland law which prohibits redisclosure or other. Employee benefits division, hipaa privacy officer, room 510, 301 w. Web a hipaa release form must be obtained from a patient before their protected health information is disclosed for any purpose other than those detailed in 45 cfr §164.506, which are specifically covered in 45 cfr §164.508.
Medical Records Release Form Hipaa Mahmooda Gilani
For additional information and resources, visit the mhcc cybersecurity webpage. Web patient authorization to release protected health information (phi) patient name: Web on january 25, 2013, the us department of health and human services (hhs) published the omnibus final rule, which implemented changes to hipaa pursuant to the hitech act and the genetic information nondiscrimination act (gina) of 2008. Web.
Medical Release Authorization Carolina Form South To Information Hipaa
Initial all items covered by this release. Web hipaa regulations require that patient documents must be kept a minimum of six (6) years. At request of individual other: Keep it simple when filling out your maryland hipaa medical authorization release form pdf and use pdfsimpli. You must continue on the next page authorization form for release of records and information.
Free Medical Records Release Authorization Forms (HIPAA)
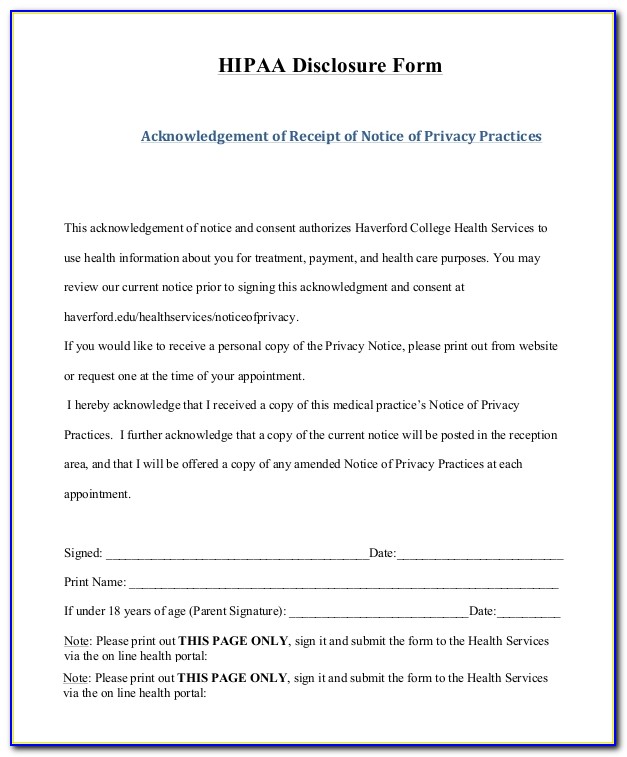
We will process your request within 10 business days of receipt. All items on this form have been completed and my questions about this form have been answered. _____ acknowledgment of receipt of services _____ complete program record (includes all items below). As the employee and holder of the. A medical release form can be revoked or reassigned at any.
HIPAA Release Form in Word and Pdf formats
If you are initiating the request for sharing information and do not wish to list the reasons for sharing, write ‘at my request’. All items on this form have been completed and my questions about this form have been answered. Web patient authorization to release protected health information (phi) patient name: Initial all items covered by this release. All items.
Hipaa Release Form Example
All items on this form have been completed and my questions about this form have been answered. Web iac compliance privacy and hipaa institutional review board (irb) mdh records management office strategic data initiative (sdi) privacy and hipaa mdh privacy matters are handled through the privacy officer within iac's compliance division. Employee benefits division, hipaa privacy officer, room 510, 301.
Hipaa Release Form Ny Fill Online, Printable, Fillable, Blank pdfFiller
Please include your name in the subject line. Web the hipaa law was enacted to ensure your healthcare information remains private. Web the medical record information release (hipaa) form allows a patient to give authorization to a 3rd party and access their health records. Web patient authorization to release protected health information (phi) patient name: Hereby authorize the disclosure and.
FREE 11+ Sample HIPAA Release Forms in PDF MS Word
Cy21 pa group hipaa authorization form author: For additional information and resources, visit the mhcc cybersecurity webpage. We will process your request within 10 business days of receipt. Web by signing this form, i either wish to file a complaint, or i authorize a health care provider to file a complaint on my behalf, with the health education and advocacy.
FREE 11+ Sample HIPAA Release Forms in PDF MS Word
Web the hipaa law was enacted to ensure your healthcare information remains private. Keep a copy of this completed form for your records. Keep it simple when filling out your maryland hipaa medical authorization release form pdf and use pdfsimpli. Web on january 25, 2013, the us department of health and human services (hhs) published the omnibus final rule, which.
Web This Document Compares The Similarities And Differences In Regulations Addressing Privacy Of Health Care Information Between The Maryland Confidentiality Of Medical Records Act (Mcrma) And Hipaa.
If you are initiating the request for sharing information and do not wish to list the reasons for sharing, write ‘at my request’. Web 10.reason for release of information: By signing this form, i either wish to file a complaint, or i authorize a health care provider to file a complaint on my behalf, with the health education and advocacy unit (heau) of the office of the attorney general and/or the maryland insurance administration (mia). Hipaa authorization fillable form 100914 author:
Web On January 25, 2013, The Us Department Of Health And Human Services (Hhs) Published The Omnibus Final Rule, Which Implemented Changes To Hipaa Pursuant To The Hitech Act And The Genetic Information Nondiscrimination Act (Gina) Of 2008.
If not the patient, name of person signing form: Hereby authorize the disclosure and use of my health information: Web authorization form for release of records and information page 3. All items on this authorization must be completed in full, or the request will not be honored.
Web Use A Separate Form For Each Person Or Agency With Which Information May Be Shared.
Web iac compliance privacy and hipaa institutional review board (irb) mdh records management office strategic data initiative (sdi) privacy and hipaa mdh privacy matters are handled through the privacy officer within iac's compliance division. [check as appropriate] from or to from or university of maryland university health center Authority to sign on behalf of patient: A medical release form can be revoked or reassigned at any time by the patient.
Date Or Event On Which This Authorization Will Expire:
As the employee and holder of the. _____ acknowledgment of receipt of services _____ complete program record (includes all items below). You can email us your form at ummsrelease@umm.edu. Web the hipaa law was enacted to ensure your healthcare information remains private.