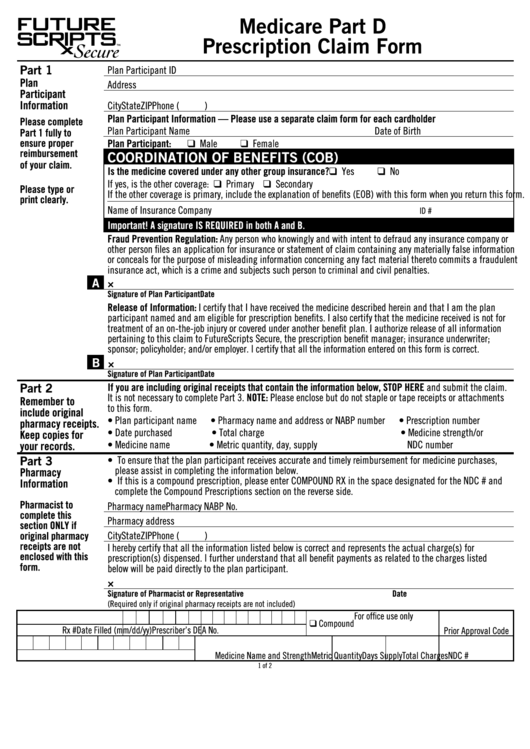
Medicare Part D Claim Form
Medicare Part D Claim Form - (2) mail the completed form and itemized bills to the correct medicare administrative contractor as indicated on pages 7 through 18 of the instructions. No part b medicare benefits may be paid unless this form is received as required by existing law and regulations. Additional information and instructions on back, please read carefully. Keep a copy of all documents submitted for your records. Complete one form per member. You may submit equivalent written documentation, but it must provide all. Do not combine claims for different members in the same fax submission. Please allow additional mail time. Do not staple or tape receipts or attachments to this form. Follow the instructions for the type of claim you're filing (listed above under how do i file a claim?).
Get all forms in alternate formats. Complete one form per member. You may submit equivalent written documentation, but it must provide all. Medicare will not process a beneficiary request for payment for diabetic test strips, part b drugs, or for items paid. Do not combine claims for different members in the same fax submission. Web medicare part d claim form use this form to request reimbursement for covered medications purchased at retail cost. No part b medicare benefits may be paid unless this form is received as required by existing law and regulations. Do not staple or tape receipts or attachments to this form. Use of the form is not required. Web reference the medicare administrative contractor address table for the correct address to mail your claim form.
Follow the instructions for the type of claim you're filing (listed above under how do i file a claim?). Complete one form per member. Please allow additional mail time. Use of the form is not required. Web the prescription drug claim form is offered as a tool to assist in getting your claim paid as soon as possible. Web prescription claim form your complete claim will be processed within 14 days of receipt of your request. Web how do i file a claim? Do not staple or tape receipts or attachments to this form. (2) mail the completed form and itemized bills to the correct medicare administrative contractor as indicated on pages 7 through 18 of the instructions. Web get forms to file a claim, set up recurring premium payments, and more.
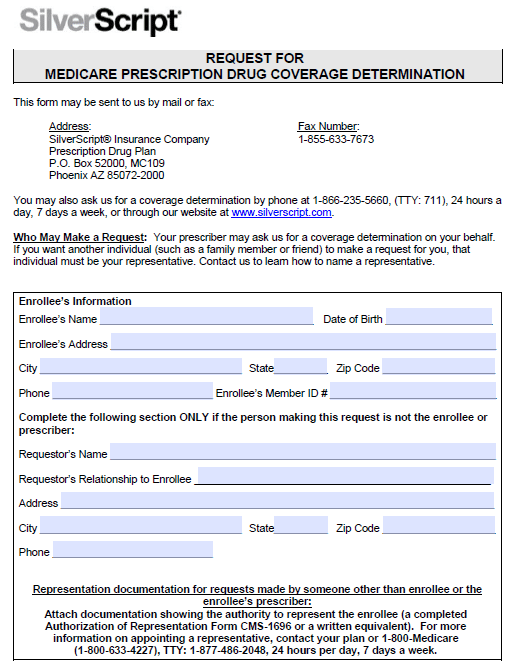
Free SilverScript Prior Prescription (Rx) Authorization Form PDF
Member information 2 physician and pharmacy information prescribing physician namedispensing pharmacy. What do i submit with the claim? No part b medicare benefits may be paid unless this form is received as required by existing law and regulations. Do not combine claims for different members in the same fax submission. Medicare will not process a beneficiary request for payment for.

Aetna Medicare Pa Forms Universal Network
Please use one claim form per fax. Claims missing information may be returned or payment may be denied mail this claim to: Medicare will not process a beneficiary request for payment for diabetic test strips, part b drugs, or for items paid. You may submit equivalent written documentation, but it must provide all. Web the prescription drug claim form is.
Medicare Form 1490s Instructions Form Resume Examples Wk9yGWvV3D
Complete one form per member. Web medicare part d claim form use this form to request reimbursement for covered medications purchased at retail cost. Get all forms in alternate formats. What do i submit with the claim? Use of the form is not required.

Central Health Medicare Plan Otc Order Form Online Form Resume
Do not staple or tape receipts or attachments to this form. Complete one form per member. Follow the instructions for the type of claim you're filing (listed above under how do i file a claim?). Please allow additional mail time. Get medicare forms for different situations, like filing a claim or appealing a coverage decision.

Aarp Medicare Part D Prior Auth Form Universal Network
Web get forms to file a claim, set up recurring premium payments, and more. Web how do i file a claim? Web the prescription drug claim form is offered as a tool to assist in getting your claim paid as soon as possible. Do not staple or tape receipts or attachments to this form. Get medicare forms for different situations,.
Medicare Part D Prescription Claim Form printable pdf download
Additional information and instructions on back, please read carefully. Web how do i file a claim? Member information 2 physician and pharmacy information prescribing physician namedispensing pharmacy. No part b medicare benefits may be paid unless this form is received as required by existing law and regulations. Web the prescription drug claim form is offered as a tool to assist.
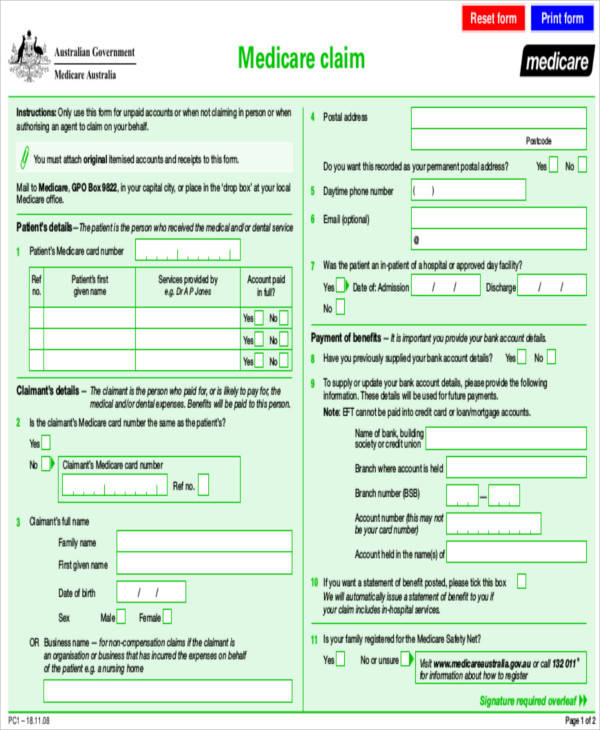
Medicare Claim Form Printable Master of Documents
Please allow additional mail time. No part b medicare benefits may be paid unless this form is received as required by existing law and regulations. Member information 2 physician and pharmacy information prescribing physician namedispensing pharmacy. Get medicare forms for different situations, like filing a claim or appealing a coverage decision. Please use one claim form per fax.

Anthem Medicare Part D Claim Form Universal Network
(2) mail the completed form and itemized bills to the correct medicare administrative contractor as indicated on pages 7 through 18 of the instructions. Additional information and instructions on back, please read carefully. You may submit equivalent written documentation, but it must provide all. Claims missing information may be returned or payment may be denied mail this claim to: No.
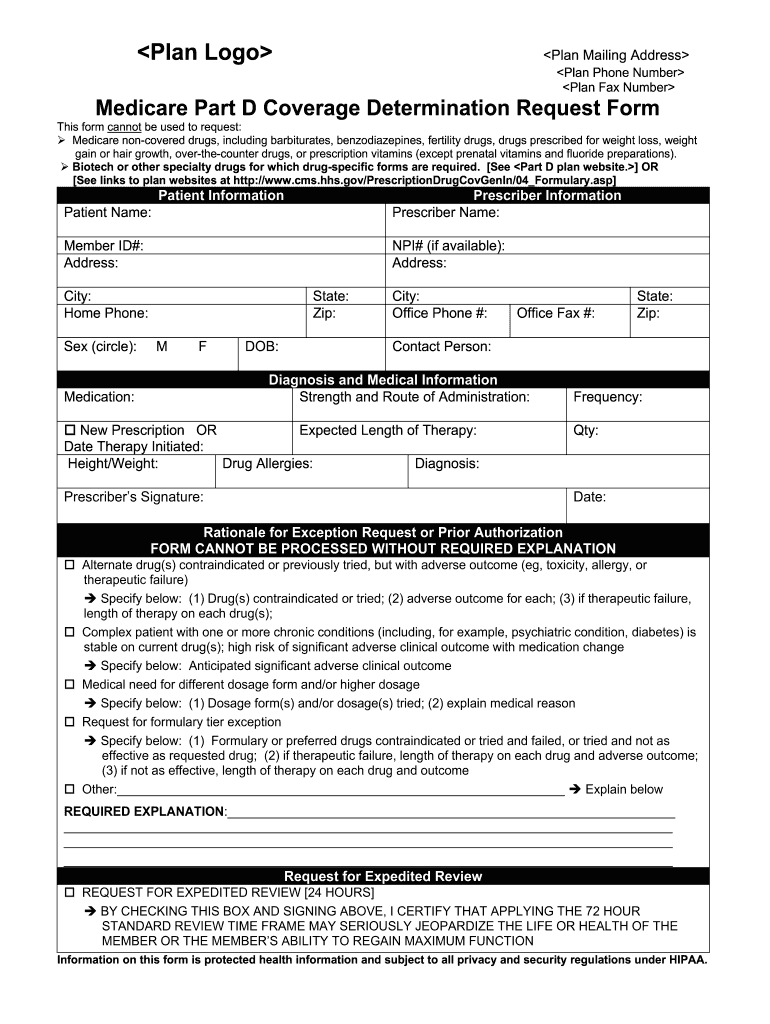
Medicare Part D Coverage Determination Form Fill Out and Sign
Follow the instructions for the type of claim you're filing (listed above under how do i file a claim?). Do not combine claims for different members in the same fax submission. Do not staple or tape receipts or attachments to this form. Web how do i file a claim? Please use one claim form per fax.

Aarp Medicare Part D Claim Form Universal Network
Web prescription claim form your complete claim will be processed within 14 days of receipt of your request. Complete one form per member. Use of the form is not required. Do not combine claims for different members in the same fax submission. Claims missing information may be returned or payment may be denied mail this claim to:
No Part B Medicare Benefits May Be Paid Unless This Form Is Received As Required By Existing Law And Regulations.
Use of the form is not required. Please use one claim form per fax. Complete one form per member. Complete one form per member.
Web Get Forms To File A Claim, Set Up Recurring Premium Payments, And More.
Keep a copy of all documents submitted for your records. What do i submit with the claim? Please allow additional mail time. You may submit equivalent written documentation, but it must provide all.
Web Reference The Medicare Administrative Contractor Address Table For The Correct Address To Mail Your Claim Form.
(2) mail the completed form and itemized bills to the correct medicare administrative contractor as indicated on pages 7 through 18 of the instructions. Do not combine claims for different members in the same fax submission. Web the prescription drug claim form is offered as a tool to assist in getting your claim paid as soon as possible. Member information 2 physician and pharmacy information prescribing physician namedispensing pharmacy.
Web Medicare Part D Claim Form Use This Form To Request Reimbursement For Covered Medications Purchased At Retail Cost.
Additional information and instructions on back, please read carefully. Claims missing information may be returned or payment may be denied mail this claim to: Get all forms in alternate formats. Do not staple or tape receipts or attachments to this form.