Optum Patient Summary Form
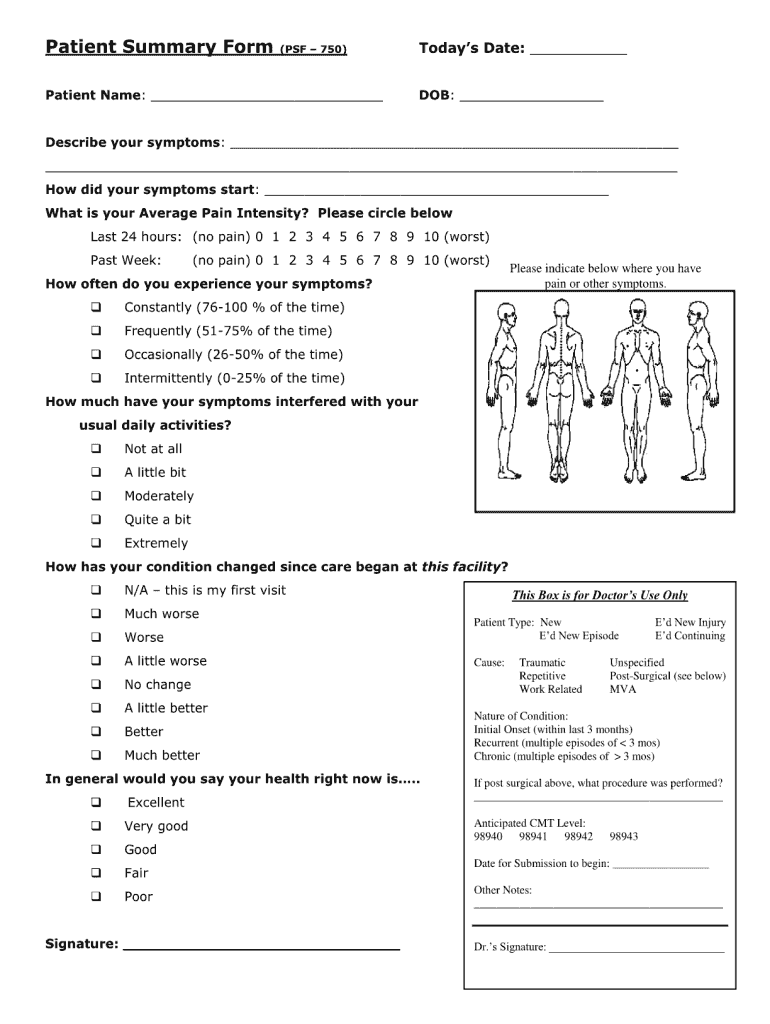
Optum Patient Summary Form - Web patient information 3 pt 4 ot date referral issued (if applicable) instructions please complete this form within the specified timeframe. Web a service representative may connect you with your assigned support clinician. Web providers contracted by optum physical health require clinical submission, which includes the plan member’s initial evaluation. Optumhealth uses this form to review patient eligibility and to enter demographic and clinical data in to our clinical information system. Manage care for your child. I am frequently encouraged to use the “online format” for patient summary form submissions. Psfs should be sent within three days 2 3 patient completes this section: Web we make it easy for you to view, download and print the forms and documents you need when seeing a doctor. Web easily manage your health care in one secure spot.
Female male 1 2 3 traumatic unspecified patient type repetitive cause of current episode 2° patient date of birth city state zip code 7. Additionally, your support clinician’s name is listed on the response to submission you receive when you submit a patient summary form. Web providers contracted by optum physical health require clinical submission, which includes the plan member’s initial evaluation. Schedule appointments with your provider. 2 3 patient completes this section: Address of the billing provider or facility indicated in box #1 8. Web a service representative may connect you with your assigned support clinician. Please review the plan summary for more information. Web we make it easy for you to view, download and print the forms and documents you need when seeing a doctor. I am frequently encouraged to use the “online format” for patient summary form submissions.
See a provider to access secure messaging. 2 3 patient completes this section: Manage care for your child. Web documented in the appropriate boxes on the patient summary form. Web providers contracted by optum physical health require clinical submission, which includes the plan member’s initial evaluation. I am frequently encouraged to use the “online format” for patient summary form submissions. Optumhealth uses this form to review patient eligibility and to enter demographic and clinical data in to our clinical information system. Web patient information 3 pt 4 ot date referral issued (if applicable) instructions please complete this form within the specified timeframe. Web we make it easy for you to view, download and print the forms and documents you need when seeing a doctor. Download and fill out the health assessment and insurance information form.

Optum Wellness Assessment Form For Youth Fill Online, Printable
Schedule appointments with your provider. 7/1/2015) patient name last first mi patient insurance id# patient address provider completes this section: Optumhealth uses this form to review patient eligibility and to enter demographic and clinical data in to our clinical information system. Please review the plan summary for more information. Submit the patient summary form within 10 days of the date.
secure patient engagement capabilities on any device
2 3 patient completes this section: Web we make it easy for you to view, download and print the forms and documents you need when seeing a doctor. Www.myoptumhealthphysicalhealth.com (registration and assistance available at: The following directions will assist in making the online submission process easy and convenient for providers and their staff Web easily manage your health care in.
Provider Express Fill Out and Sign Printable PDF Template signNow
Optumhealth uses this form to review patient eligibility and to enter demographic and clinical data in to our clinical information system. Female male 1 2 3 traumatic unspecified patient type repetitive cause of current episode 2° patient date of birth city state zip code 7. Web we make it easy for you to view, download and print the forms and.
AF IMT Form 3829 Download Fillable PDF or Fill Online Summary of
Psfs should be sent within three days The following directions will assist in making the online submission process easy and convenient for providers and their staff Optumhealth uses this form to review patient eligibility and to enter demographic and clinical data in to our clinical information system. Www.myoptumhealthphysicalhealth.com (registration and assistance available at: Additionally, your support clinician’s name is listed.
Myoptumhealthphysicalhealth Form Fill Out and Sign Printable PDF
2 3 patient completes this section: Submit the patient summary form within 10 days of the date indicated under “date you want this submission to 4 begin.” submit to optumhealth physical health via: Web providers contracted by optum physical health require clinical submission, which includes the plan member’s initial evaluation. The following directions will assist in making the online submission.

Review Patient Summary YouTube
Web a service representative may connect you with your assigned support clinician. Web patient information 3 pt 4 ot date referral issued (if applicable) instructions please complete this form within the specified timeframe. Web providers contracted by optum physical health require clinical submission, which includes the plan member’s initial evaluation. Web easily manage your health care in one secure spot..

20132021 Form OPTUMRx 1040006 Fill Online, Printable, Fillable, Blank
Web easily manage your health care in one secure spot. Additionally, your support clinician’s name is listed on the response to submission you receive when you submit a patient summary form. 2 3 patient completes this section: Manage care for your child. Www.myoptumhealthphysicalhealth.com (registration and assistance available at:
Optum Rx Pa Form Fill Out and Sign Printable PDF Template signNow
Female male 1 2 3 traumatic unspecified patient type repetitive cause of current episode 2° patient date of birth city state zip code 7. Address of the billing provider or facility indicated in box #1 8. Submit the patient summary form within 10 days of the date indicated under “date you want this submission to 4 begin.” submit to optumhealth.

20152022 Form PSF750 Fill Online, Printable, Fillable, Blank pdfFiller
7/1/2015) patient name last first mi patient insurance id# patient address provider completes this section: Web a service representative may connect you with your assigned support clinician. Manage care for your child. Submit the patient summary form within 10 days of the date indicated under “date you want this submission to 4 begin.” submit to optumhealth physical health via: See.

Psf form Fill out & sign online DocHub
I am frequently encouraged to use the “online format” for patient summary form submissions. After the initial visit, care providers must complete and submit a patient summary form (psf) through optumhealth physical health’s website at: 7/1/2015) patient name last first mi patient insurance id# patient address provider completes this section: Web a service representative may connect you with your assigned.
Psfs Should Be Sent Within Three Days
Download and fill out the health assessment and insurance information form. Web documented in the appropriate boxes on the patient summary form. See a provider to access secure messaging. Web providers contracted by optum physical health require clinical submission, which includes the plan member’s initial evaluation.
Please Review The Plan Summary For More Information.
Female male 1 2 3 traumatic unspecified patient type repetitive cause of current episode 2° patient date of birth city state zip code 7. Optumhealth uses this form to review patient eligibility and to enter demographic and clinical data in to our clinical information system. Submit the patient summary form within 10 days of the date indicated under “date you want this submission to 4 begin.” submit to optumhealth physical health via: Manage care for your child.
The Following Directions Will Assist In Making The Online Submission Process Easy And Convenient For Providers And Their Staff
Www.myoptumhealthphysicalhealth.com (registration and assistance available at: 7/1/2015) patient name last first mi patient insurance id# patient address provider completes this section: Address of the billing provider or facility indicated in box #1 8. 2 3 patient completes this section:
Web Patient Information 3 Pt 4 Ot Date Referral Issued (If Applicable) Instructions Please Complete This Form Within The Specified Timeframe.
Additionally, your support clinician’s name is listed on the response to submission you receive when you submit a patient summary form. Web easily manage your health care in one secure spot. Web we make it easy for you to view, download and print the forms and documents you need when seeing a doctor. Schedule appointments with your provider.