Prescription Request Form
Prescription Request Form - Patients can enter multiple prescriptions on the same form using. This specialty pharmacy may contact you regarding paragard, or you may contact them. Web enter the patient and health care provider information in the space provided on the prescription request form including the patient’s pharmacy drug benefit and medical. An enrollee or an enrollee's representative may use this model form to request a reconsideration with. Web expenses related to prescription orders. Web use our free prescription refill request form template to allow patients to easily request prescriptions online. If your doctor can establish medical. Web inbrija ® prescription reuest form fax completed form to: Use nabp 3677361 to send. Universal pharmacy benefit drug authorization form;
Web we offer access to specialty medications and infusion therapies, centralized intake and benefits verification, and prior authorization assistance. By supplying my credit card number, i authorize optum rx to maintain my credit card on file as payment method for any future charges. Web this prescription form can be used by physicians and medical practices to provide patients with an easy, accessible, and secure prescription when they need it. Covermymeds® is a free service that allows. Web our prescription refill request form template is used to request prescriptions online by patients. Web prescription benefit plan may request additional information or clarification, if needed, to evaluate requests. Web inbrija ® prescription reuest form fax completed form to: This template contains information about the patient’s name, phone number and. Web up to $40 cash back the express scripts claim form is a document used to submit a request for reimbursement of prescription medication expenses to express scripts, a pharmacy. Web expenses related to prescription orders.
This specialty pharmacy may contact you regarding paragard, or you may contact them. By supplying my credit card number, i authorize optum rx to maintain my credit card on file as payment method for any future charges. Web this prescription form can be used by physicians and medical practices to provide patients with an easy, accessible, and secure prescription when they need it. Web we offer access to specialty medications and infusion therapies, centralized intake and benefits verification, and prior authorization assistance. Web patients may apply to lilly cares to receive prescribed lilly oncology medications by completing an online or printable application form at www.lillycares.com. If your doctor can establish medical. Web elixir pharmacy 7835 freedom avenue nw north canton, oh 44720 toll free: An enrollee or an enrollee's representative may use this model form to request a reconsideration with. Records are retained in accordance with state board of pharmacy, dea, and. Web inbrija ® prescription reuest form fax completed form to:
14+ Prescription Templates Doctor Pharmacy Medical
This template contains information about the patient’s name, phone number and. This specialty pharmacy may contact you regarding paragard, or you may contact them. Web use this form to order a new mail service prescription by fax from the prescriber's office mail order prescription physician fax form before you send us a prescription and to. Web patients may apply to.
Prior Authorization Request Form For Specialty Prescription Drugs Us
An enrollee or an enrollee's representative may use this model form to request a reconsideration with. Web if your request for records is in excess of fifteen (15) months, please indicate the time frame below. Web our prescription refill request form template is used to request prescriptions online by patients. Web use this form to order a new mail service.

Continence Prescription Request Form 2015
Web we offer access to specialty medications and infusion therapies, centralized intake and benefits verification, and prior authorization assistance. Web inbrija ® prescription reuest form fax completed form to: Web if your request for records is in excess of fifteen (15) months, please indicate the time frame below. Web use this form to order a new mail service prescription by.

How to Order Repeat Prescriptions Padiham Medical Centre
Web use this form to order a new mail service prescription by fax from the prescriber's office mail order prescription physician fax form before you send us a prescription and to. Web your healthcare provider has ordered paragard through the following specialty pharmacy. Web this prescription form can be used by physicians and medical practices to provide patients with an.
Request For Medicare Prescription Drug Coverage Determination Form
Web enter the patient and health care provider information in the space provided on the prescription request form including the patient’s pharmacy drug benefit and medical. The selected specialty pharmacy makes no assurance that any prescribed drug will be covered or reimbursed at any specific level under any patient’s insurance plan, or. Web use our free prescription refill request form.
RX1 Prescription Pad Positive Impressions
Covermymeds® is a free service that allows. Web up to $40 cash back the express scripts claim form is a document used to submit a request for reimbursement of prescription medication expenses to express scripts, a pharmacy. Web use our free prescription refill request form template to allow patients to easily request prescriptions online. Web request for reconsideration of medicare.
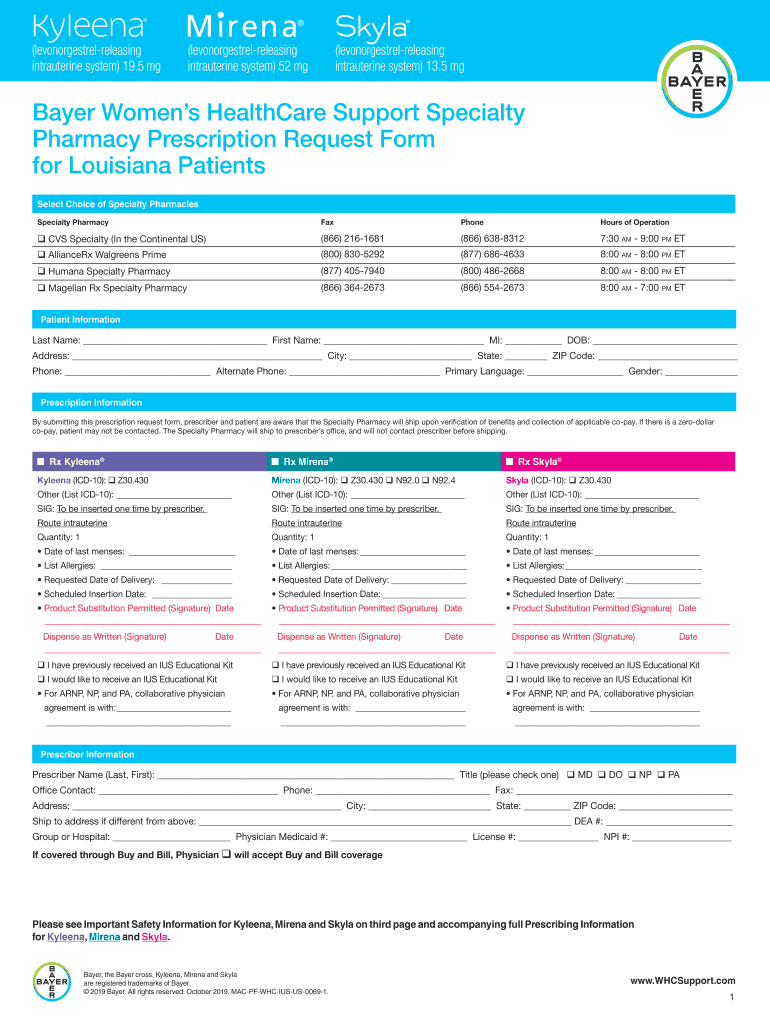
Bayer Women's Healthcare Support Specialty Pharmacy Prescription
Web prescribers can submit their requests to humana clinical pharmacy review (hcpr) in the following ways: This template contains information about the patient’s name, phone number and. Web we offer access to specialty medications and infusion therapies, centralized intake and benefits verification, and prior authorization assistance. The selected specialty pharmacy makes no assurance that any prescribed drug will be covered.

REPEAT PRESCRIPTION REQUEST FORM
Universal pharmacy benefit drug authorization form; Web we offer access to specialty medications and infusion therapies, centralized intake and benefits verification, and prior authorization assistance. Web elixir pharmacy 7835 freedom avenue nw north canton, oh 44720 toll free: Use nabp 3677361 to send. Web use this form to order a new mail service prescription by fax from the prescriber's office.
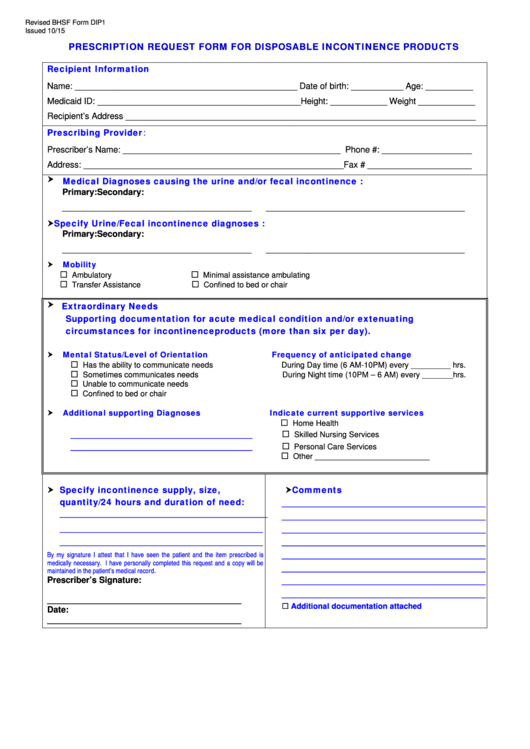
Bhsf Form Dip1 Prescription Request Form For Disposable Incontinence
The selected specialty pharmacy makes no assurance that any prescribed drug will be covered or reimbursed at any specific level under any patient’s insurance plan, or. This template contains information about the patient’s name, phone number and. Web if your request for records is in excess of fifteen (15) months, please indicate the time frame below. Web our prescription refill.
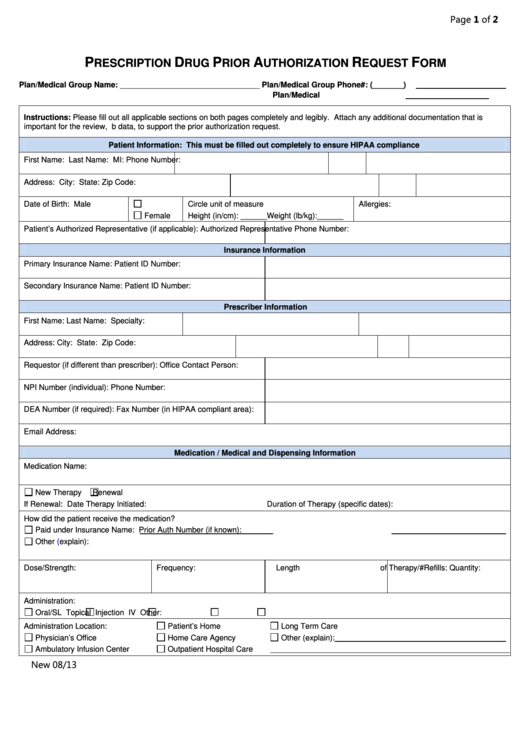
Fillable Prescription Drug Prior Authorization Request Form printable
Use nabp 3677361 to send. If your doctor can establish medical. Web we offer access to specialty medications and infusion therapies, centralized intake and benefits verification, and prior authorization assistance. Covermymeds® is a free service that allows. An enrollee or an enrollee's representative may use this model form to request a reconsideration with.
Web This Prescription Form Can Be Used By Physicians And Medical Practices To Provide Patients With An Easy, Accessible, And Secure Prescription When They Need It.
By supplying my credit card number, i authorize optum rx to maintain my credit card on file as payment method for any future charges. Web use our free prescription refill request form template to allow patients to easily request prescriptions online. Patients can enter multiple prescriptions on the same form using. Web if your request for records is in excess of fifteen (15) months, please indicate the time frame below.
If Your Doctor Can Establish Medical.
Covermymeds® is a free service that allows. Web use this form to order a new mail service prescription by fax from the prescriber's office mail order prescription physician fax form before you send us a prescription and to. An enrollee or an enrollee's representative may use this model form to request a reconsideration with. Web expenses related to prescription orders.
The Selected Specialty Pharmacy Makes No Assurance That Any Prescribed Drug Will Be Covered Or Reimbursed At Any Specific Level Under Any Patient’s Insurance Plan, Or.
Web inbrija ® prescription reuest form fax completed form to: This specialty pharmacy may contact you regarding paragard, or you may contact them. Web your healthcare provider has ordered paragard through the following specialty pharmacy. Web specialty prescription referral form;
Use Nabp 3677361 To Send.
Web our prescription refill request form template is used to request prescriptions online by patients. Web elixir pharmacy 7835 freedom avenue nw north canton, oh 44720 toll free: Universal pharmacy benefit drug authorization form; This template contains information about the patient’s name, phone number and.