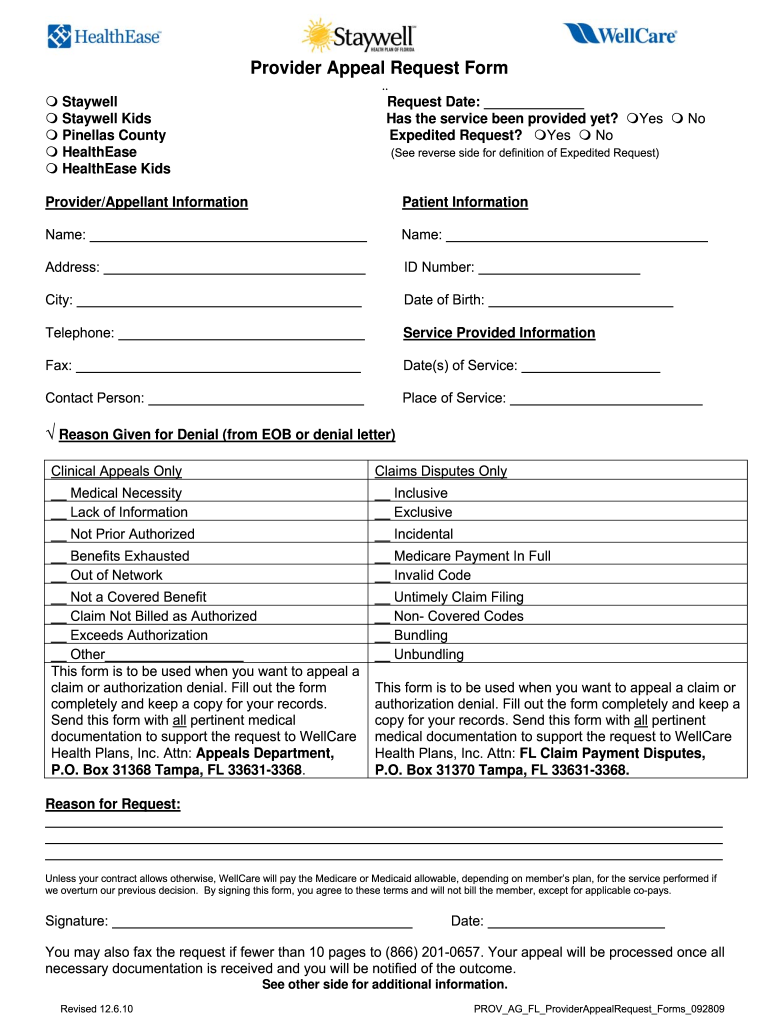
Wellcare Provider Payment Dispute Request Form
Wellcare Provider Payment Dispute Request Form - Web up to $40 cash back fill wellcare provider payment dispute request form, edit online. You can also download it, export it or print it out. Web send this form with full pertinent medical documentation to support the request to wellcare attn: Web send this form with all pertinent medical documentation to support the request to wellcare health plans, inc. Complete all necessary information in the. By continuing to use our site, you agree to our privacy policy and terms of use. Web english home health services request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english hospice authorization request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english inpatient request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english. Sign, fax and printable from pc, ipad, tablet or mobile with pdffiller instantly. Experience all the benefits of completing and submitting forms online. Send this form with all pertinent medical documentation to.
Web up to $40 cash back fill wellcare provider payment dispute request form, edit online. By continuing to use our site, you agree to our privacy policy and terms of use. Complete all necessary information in the. Access key forms for authorizations,. Primarily address utilization management authorization denials in addition to claim. Web english home health services request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english hospice authorization request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english inpatient request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english. With our service completing wellcare provider payment. Edit, sign and save wellcare payment dispute req form. Web comply with our easy steps to have your wellcare payment dispute form prepared rapidly: Edit your wellcare payment dispute form online.
Authorizations · delivery notification form ( pdf) · dme authorization request form ( pdf) · home health. Web follow the simple instructions below: Web a repository of medicare forms and documents for wellcare supporters, covering our such for authorizations, requirements and behavioral health. Web up to $40 cash back wellcare provider appeal request is a document that healthcare providers can use to request reconsideration of a claim that has been denied or disputed. By continuing to use our site, you agree to our privacy policy and terms of use. Primarily address utilization management authorization denials in addition to claim. Web clinical appeals can be submitted thru our provider portal electronically. Register and subscribe now to work on your wellcare provider payment dispute request form. Web notice of pregnancy form (pdf) provider incident report form (pdf) pcp change request form for prepaid health plans (phps) (pdf) provider referral form: Web english home health services request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english hospice authorization request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english inpatient request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english.
Wellcare Appeal Form Pdf Fill Online, Printable, Fillable, Blank
Web disputes, reconsiderations and grievances. With our service completing wellcare provider payment. You can also download it, export it or print it out. Pick the template in the catalogue. Authorizations · delivery notification form ( pdf) · dme authorization request form ( pdf) · home health.
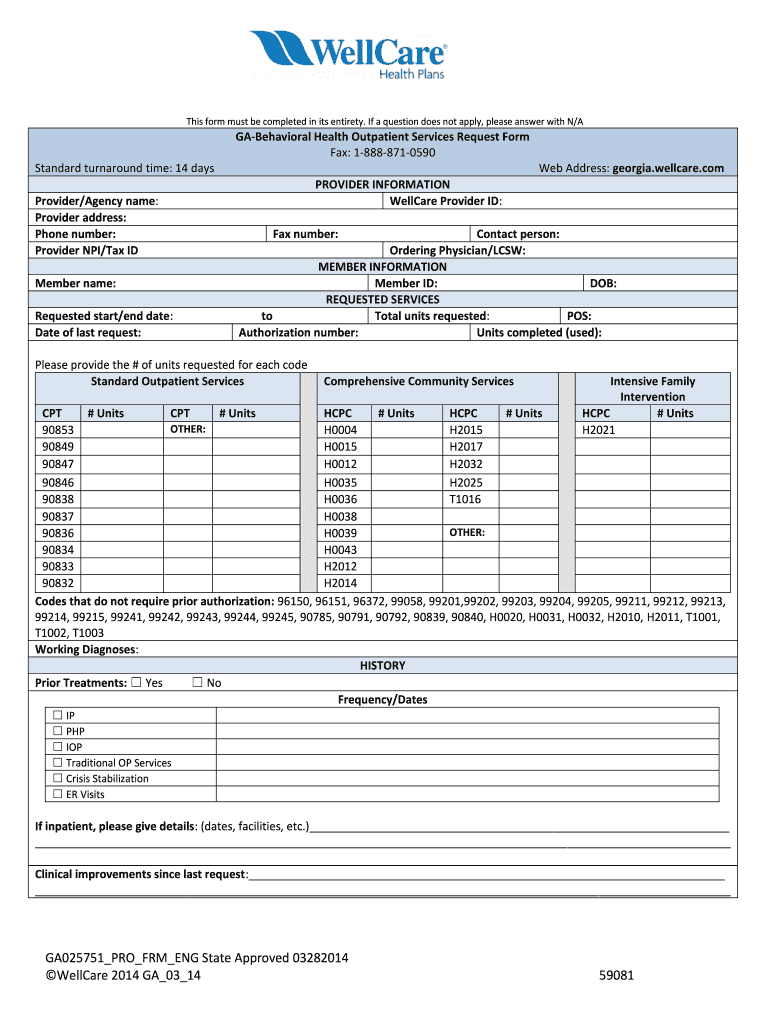
Wellcare Behavioral Health Service Request Form Fill Out and Sign
Web • a claim dispute (level ii) should be used only when a provider has received an unsatisfactory response to a request for reconsideration. Authorizations · delivery notification form ( pdf) · dme authorization request form ( pdf) · home health. Web send wellcare claim dispute form via email, link, or fax. Register and subscribe now to work on your.

Welcare Medicare Prior Authorization Form For Medication Fill Online
Experience all the benefits of completing and submitting forms online. Use get form or simply click on the template preview to open it in the editor. Web up to $40 cash back fill wellcare provider payment dispute request form, edit online. Primarily address utilization management authorization denials in addition to claim. Pick the template in the catalogue.

wellcare reimbursement form Fill out & sign online DocHub
Ad register and subscribe now to work on your wellcare provider payment dispute request form. Authorizations · delivery notification form ( pdf) · dme authorization request form ( pdf) · home health. Web make a payment. Pick the template in the catalogue. Edit your wellcare payment dispute form online.
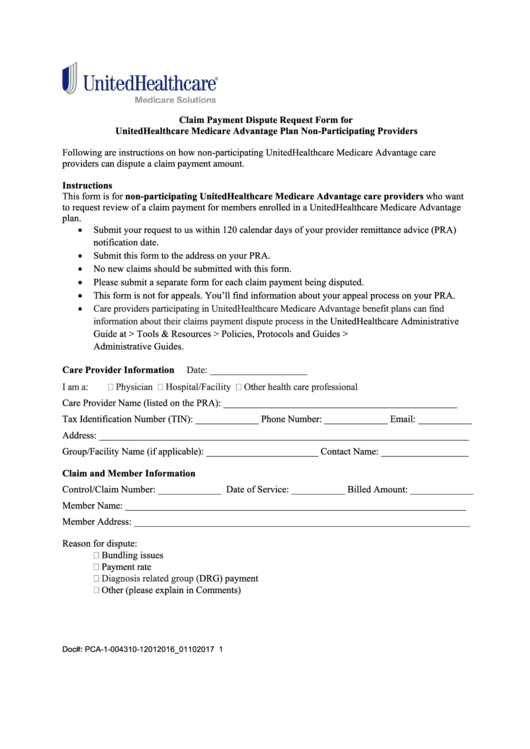
Fillable Claim Payment Dispute Request Form For Unitedhealthcare
Use get form or simply click on the template preview to open it in the editor. Web up to $40 cash back fill wellcare provider payment dispute request form, edit online. Web comply with our easy steps to have your wellcare payment dispute form prepared rapidly: Send this form with all pertinent medical documentation to. Web disputes, reconsiderations and grievances.
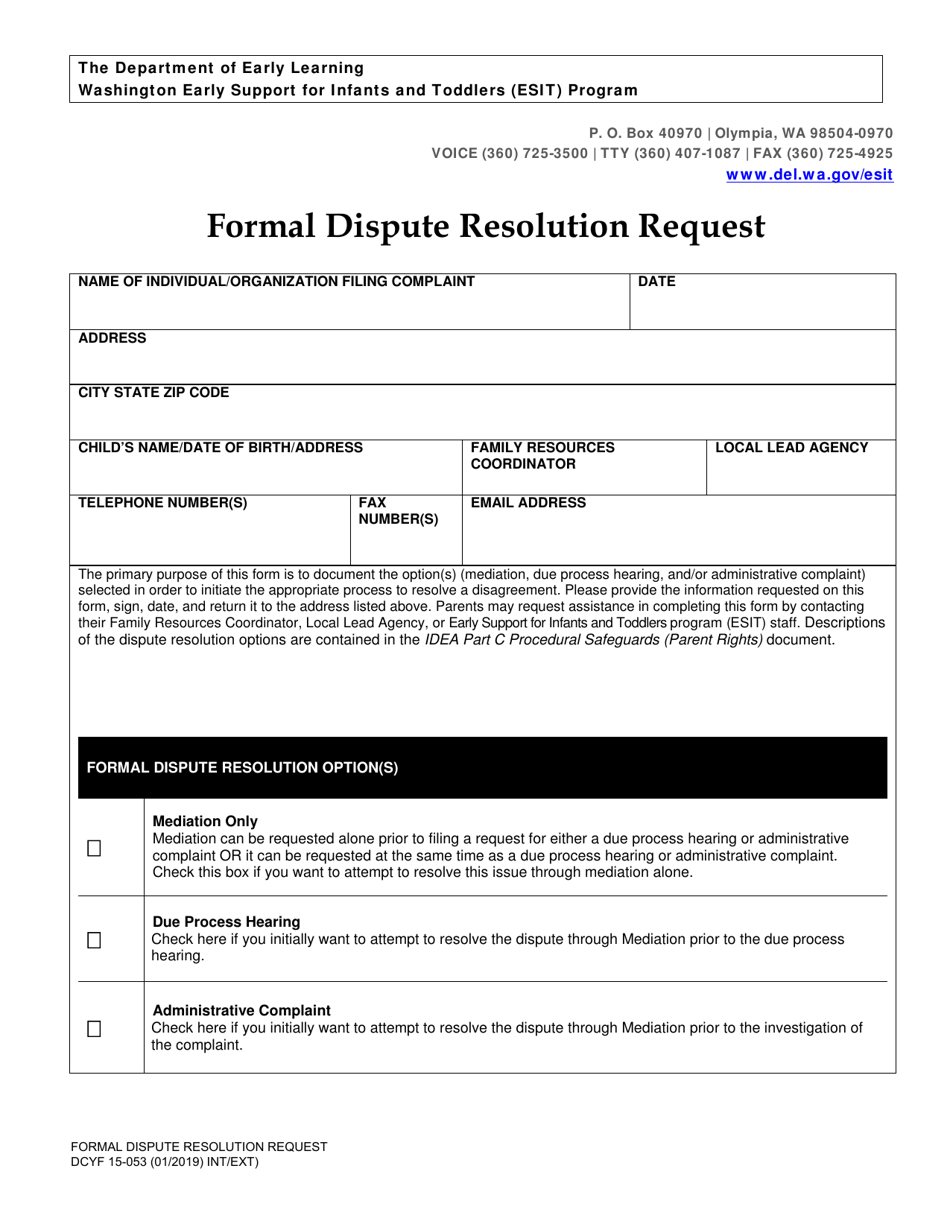
DCYF Form 15053 Download Printable PDF or Fill Online Formal Dispute
Web make a payment. Web up to $40 cash back wellcare provider appeal request is a document that healthcare providers can use to request reconsideration of a claim that has been denied or disputed. Experience all the benefits of completing and submitting forms online. Pick the template in the catalogue. Edit, sign and save wellcare payment dispute req form.
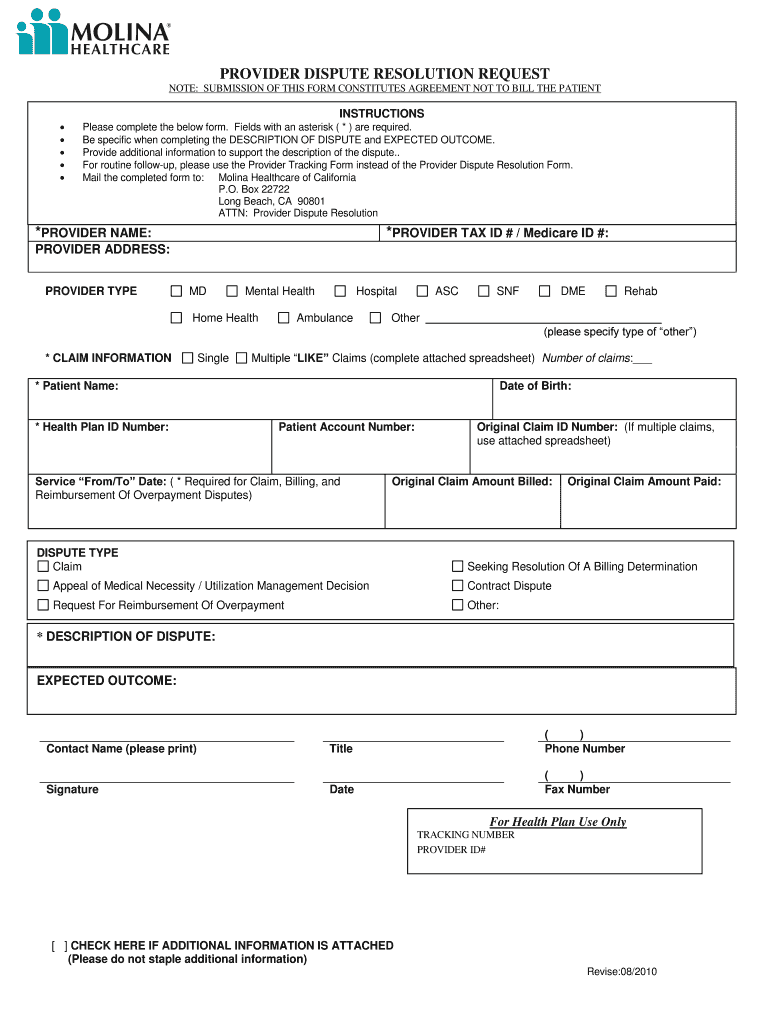
Molina Appeal Form Fill Out and Sign Printable PDF Template signNow
Complete all necessary information in the. Pick the template in the catalogue. Edit, sign and save wellcare payment dispute req form. Web comply with our easy steps to have your wellcare payment dispute form prepared rapidly: Sign, fax and printable from pc, ipad, tablet or mobile with pdffiller instantly.
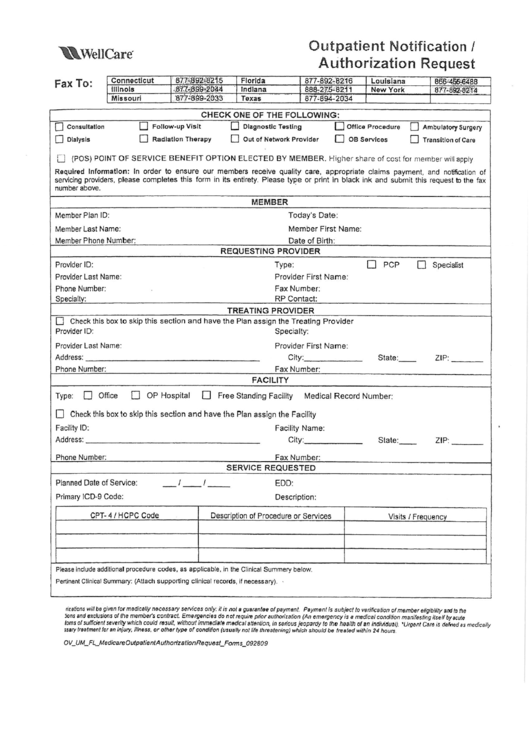
Fillable Outpatient Notification /authorization Request Wellcare
Web • a claim dispute (level ii) should be used only when a provider has received an unsatisfactory response to a request for reconsideration. Web send wellcare claim dispute form via email, link, or fax. Web a repository of medicare forms and documents for wellcare supporters, covering our such for authorizations, requirements and behavioral health. Pick the template in the.
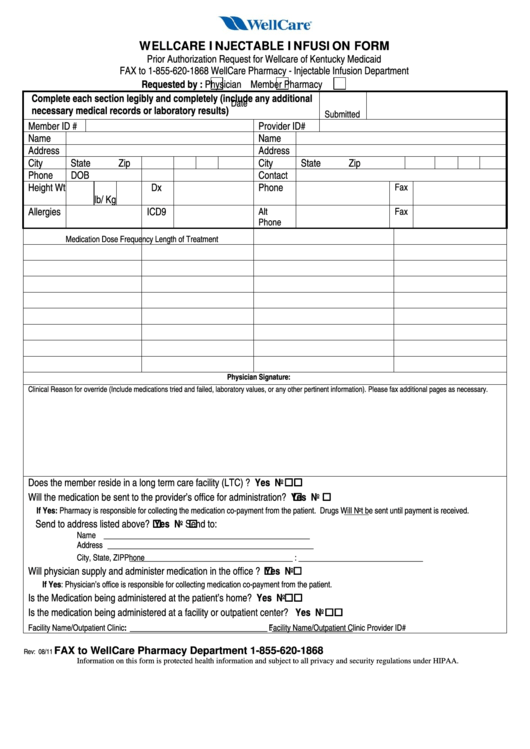
Fillable Wellcare Injectable Infusion Form Prior Authorization
Ad register and subscribe now to work on your wellcare provider payment dispute request form. Send this form with all pertinent medical documentation to. You can also download it, export it or print it out. By continuing to use our site, you agree to our privacy policy and terms of use. Complete all necessary information in the.
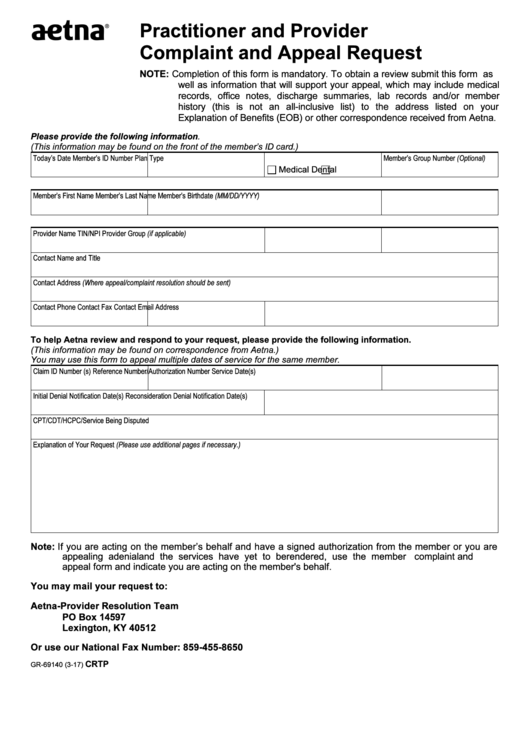
Fillable Form Gr69140 Aetna Practitioner And Provider Complaint And
Pick the template in the catalogue. Web • a claim dispute (level ii) should be used only when a provider has received an unsatisfactory response to a request for reconsideration. Web notice of pregnancy form (pdf) provider incident report form (pdf) pcp change request form for prepaid health plans (phps) (pdf) provider referral form: Authorizations · delivery notification form (.
Register And Subscribe Now To Work On Your Wellcare Provider Payment Dispute Request Form.
Web • a claim dispute (level ii) should be used only when a provider has received an unsatisfactory response to a request for reconsideration. By continuing to use our site, you agree to our privacy policy and terms of use. You can also download it, export it or print it out. Web comply with our easy steps to have your wellcare payment dispute form prepared rapidly:
Edit Your Wellcare Payment Dispute Form Online.
Ad register and subscribe now to work on your wellcare provider payment dispute request form. Experience all the benefits of completing and submitting forms online. Access key forms for authorizations,. Authorizations · delivery notification form ( pdf) · dme authorization request form ( pdf) · home health.
Web Follow The Simple Instructions Below:
Web send this form with all pertinent medical documentation to support the request to wellcare health plans, inc. Use get form or simply click on the template preview to open it in the editor. Web disputes, reconsiderations and grievances. Web clinical appeals can be submitted thru our provider portal electronically.
Sign, Fax And Printable From Pc, Ipad, Tablet Or Mobile With Pdffiller Instantly.
Web english home health services request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english hospice authorization request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english inpatient request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english. Web send this form with full pertinent medical documentation to support the request to wellcare attn: Web notice of pregnancy form (pdf) provider incident report form (pdf) pcp change request form for prepaid health plans (phps) (pdf) provider referral form: Complete all necessary information in the.